Crash of a Learjet 45 in Batesville
Date & Time:
Nov 29, 2022 at 1910 LT
Operator:

Registration:
N988MC
Survivors:
Yes
Schedule:
Waterloo – Batesville
MSN:
45-352
YOM:
2007
Flight number:
DHR003
Crew on board:
2
Crew fatalities:
Pax on board:
6
Pax fatalities:
Other fatalities:
Total fatalities:
0
Captain / Total hours on type:
1560.00
Copilot / Total hours on type:
263
Aircraft flight hours:
2490
Circumstances:
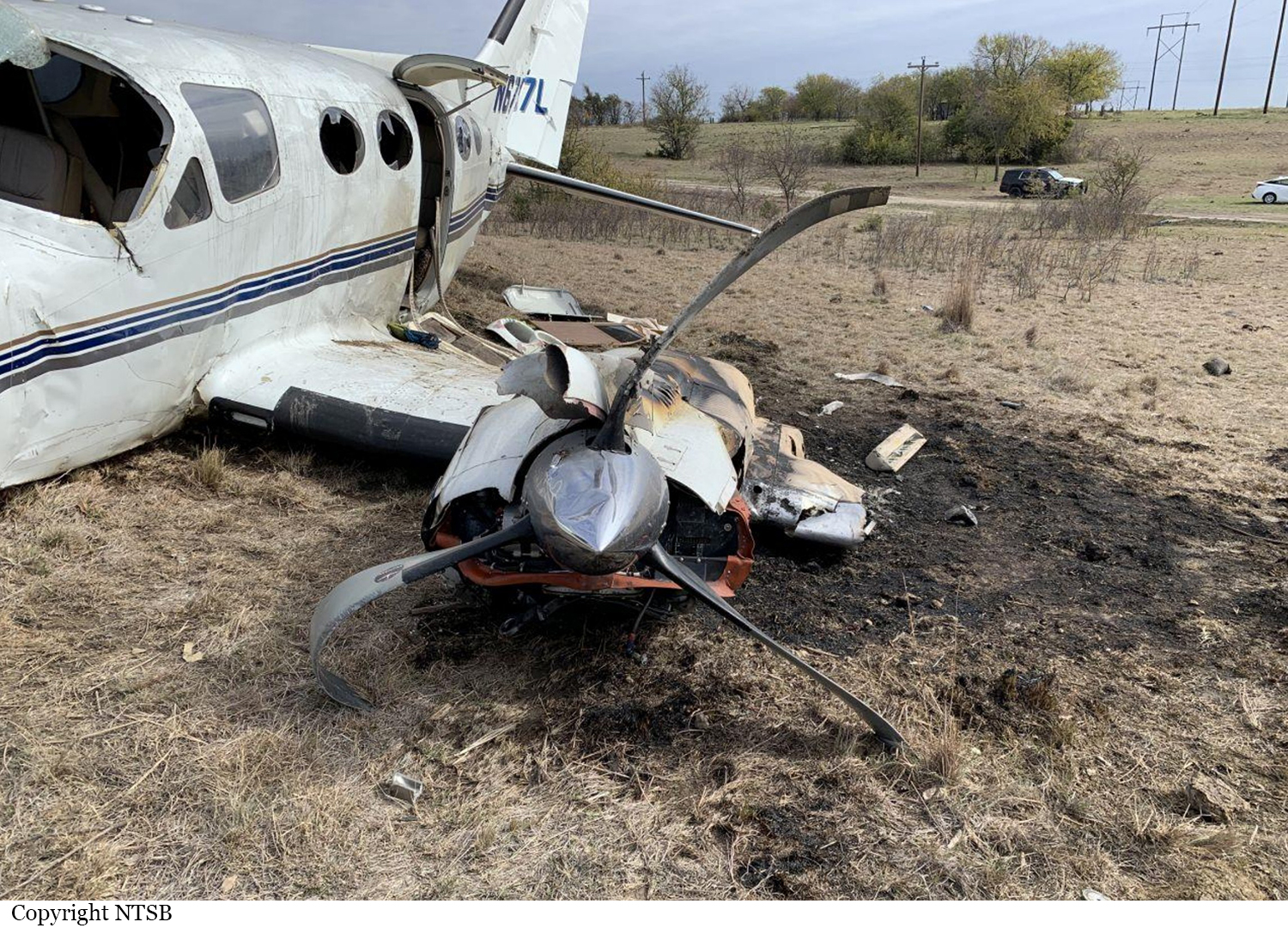
The two pilots were conducting a business flight with six passengers when the accident occurred. During the night arrival the captain flew a visual approach with excessive airspeed
and the airplane crossed the runway threshold more than 50 knots above approach speed (Vref). The before-landing checklist was not completed, and the flaps were at an incorrect 20° position instead of 40°. The airplane touched down near the midfield point of the 6,022 ft non grooved runway, which was wet due to earlier precipitation. The captain initially applied intermittent braking, then applied continuous braking starting about 2,069 ft from the end of the runway. The captain did not deploy the thrust reversers. The airplane exited the runway above 100 knots ground speed, then continued into a ditch and airport perimeter fence, which resulted in substantial damage to the forward fuselage. Examination of the airplane revealed no mechanical anomalies that would have precluded normal operation. The operator’s flight manual directed that all approaches were to be flown using the stabilized approach concept. For a visual approach, this included establishing and maintaining the proper approach speed and correct landing configuration at least 500 ft above the airport elevation. Neither pilot recognized the requirement to execute a go-around due to the excessive approach speed or the long landing on a wet runway, which resulted in the runway excursion.
and the airplane crossed the runway threshold more than 50 knots above approach speed (Vref). The before-landing checklist was not completed, and the flaps were at an incorrect 20° position instead of 40°. The airplane touched down near the midfield point of the 6,022 ft non grooved runway, which was wet due to earlier precipitation. The captain initially applied intermittent braking, then applied continuous braking starting about 2,069 ft from the end of the runway. The captain did not deploy the thrust reversers. The airplane exited the runway above 100 knots ground speed, then continued into a ditch and airport perimeter fence, which resulted in substantial damage to the forward fuselage. Examination of the airplane revealed no mechanical anomalies that would have precluded normal operation. The operator’s flight manual directed that all approaches were to be flown using the stabilized approach concept. For a visual approach, this included establishing and maintaining the proper approach speed and correct landing configuration at least 500 ft above the airport elevation. Neither pilot recognized the requirement to execute a go-around due to the excessive approach speed or the long landing on a wet runway, which resulted in the runway excursion.
Probable cause:
The crew’s failure to execute a go-around during the unstable approach and long landing, which resulted in a runway excursion.
Final Report: