Crash of a Rockwell Gulfstream 695A Jetprop 1000 near Cloncurry: 3 killed
Date & Time:
Nov 4, 2023 at 1430 LT
Operator:

Registration:
VH-HPY
Survivors:
No
Schedule:
Toowoomba - Mount Isa
MSN:
96051
YOM:
1982
Flight number:
Birddog 370
Crew on board:
1
Crew fatalities:
Pax on board:
2
Pax fatalities:
Other fatalities:
Total fatalities:
3
Captain / Total hours on type:
102.00
Aircraft flight hours:
7566
Circumstances:
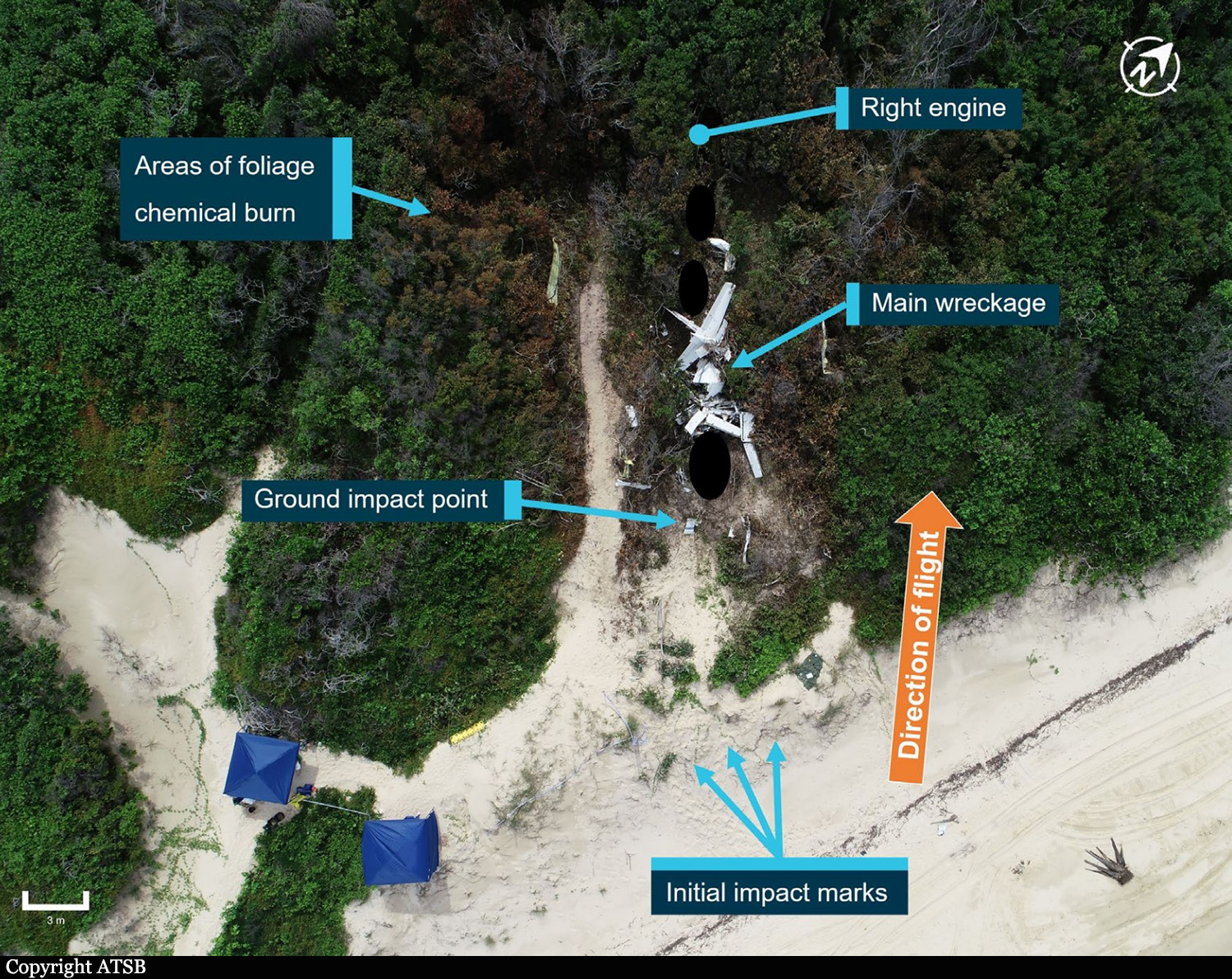
On the morning of 4 November 2023, a Gulfstream 695A, registered VH-HPY, was being operated by AGAIR on an instrument flight rules flight from Toowoomba to Mount Isa, Queensland. On board the aircraft were the pilot and 2 camera operators. The purpose of the flight was to conduct line scanning of fire zones located north of Mount Isa. About 1 hour and 50 minutes into the flight, while the aircraft was in cruise at flight level 280, air traffic control (ATC) lost radio contact with the pilot. Over the following 30 minutes, ATC made multiple attempts to re-establish contact, including using alternate frequencies and relaying messages via other aircraft in the vicinity. VH-HPY was observed diverging from track and ATC declared an uncertainty phase for the aircraft. About 20 minutes later, ATC called the pilot’s mobile telephone, and a brief conversation took place. During the conversation, the pilot’s speech was observed as slow and flat. In response, ATC upgraded the aircraft’s status to an alert phase and initiated their hypoxic pilot emergency procedures. About 10 minutes later, the crew of a nearby aircraft was able to establish contact with the pilot, having been requested to do so by ATC. The alert phase was downgraded to an uncertainty phase and, a short time later, ATC re-established direct contact with the pilot. The uncertainty phase was cancelled 1 minute later. The pilot confirmed that their oxygen system was operating normally, and they were issued a clearance to undertake line scanning north of Mount Isa. Over the following 4 minutes, the pilot repeated the clearance from ATC 4 times, seeming uncertain about the status of the clearance. The radio recordings during this period indicate that the pilot’s rate and volume of speech had substantially lowered from earlier communications and was worsening. The pilot’s final radio transmission displayed the slowest speaking rate of all their communications during the flight and contained stuttering and operational mistakes. Air traffic control did not attempt to re-establish contact with the pilot until about 18 minutes later, however no further responses from the pilot were received. A short time later, the aircraft departed controlled flight, initially entering a descending anticlockwise turn with an increasing rate of descent. At about 10,500 ft, the aircraft likely transitioned into an aerodynamic spin, with a subsequent average rate of descent of about 13,500 ft/min. The aircraft collided with terrain 55 km south-east of Cloncurry. The 3 occupants were fatally injured, and the aircraft was destroyed by impact forces and a fuel-fed post-impact fire.
Probable cause:
Contributing factors
- The pilot's ability to safely operate the aircraft was almost certainly significantly degraded by the onset of altitude hypoxia.
- While in cruise at flight level 280, both power levers were probably reduced without an appropriate descent rate being initiated, resulting in a progressive reduction of airspeed.
- The aircraft entered a descending anticlockwise turn with an increasing rate of descent. At about 10,500 ft, control input(s) were almost certainly made, probably an attempt to recover, that transitioned the aircraft from a high-speed descent to a spin condition that was likely unrecoverable and which continued until the impact with terrain.
- The pilot had a normalized practice of operating VH-HPY with a cabin altitude that required the use of supplemental oxygen. These flights were conducted without access to a suitable oxygen supply, significantly increasing the risk of altitude hypoxia induced incapacitation.
- The aircraft's pressurization system probably did not attain the required cabin altitude when operating at flight level 280 during the accident flight. The pilot probably knowingly continued the flight with a cabin altitude that required the use of supplemental oxygen, without access to a suitable oxygen supply.
- The AGAIR aircraft VH-HPY pressurization system could not reliably attain the required cabin altitude during flight due to a known, long-term, unresolved intermittent defect. AGAIR management personnel were aware of the defect and, through a combination of inaction, encouragement and, in some instances direct involvement, permitted the aircraft to continue operations at an excessive cabin altitude. (Safety issue)
- AGAIR management exercised ineffective operational control over the line scanning activities. As a result, the ongoing intermittent pressurization defect was not formally recorded, the issues with the aircraft were not communicated to the AGAIR safety manager, and the hazardous practice of operating the aircraft at a cabin altitude that required the use of supplemental oxygen, without access to a suitable oxygen supply, was allowed to continue. (Safety issue)
- The AGAIR head of flying operations did not communicate critical safety information about the known intermittent pressurization defect on VH-HPY when they were phoned by air traffic control about concerns that the pilot may be impacted by hypoxia.
- After being told by the pilot that operations were normal, controllers likely reduced their vigilance about hypoxia and did not re-identify the possibility of hypoxia during the subsequent progressive deterioration of the pilot’s speech.
Other factors that increased risk:
- AGAIR Gulfstream 690 and 695 aircraft were operated with known defects without being recorded on the aircraft’s maintenance releases, likely as a routine practice. For VH-HPY, the absence of documented historical information limited the ability to assess the operational impact of the pressurization defect and the effectiveness of maintenance rectification activities. (Safety issue)
- The Airservices Australia hypoxic pilot emergency checklist did not contain guidance on ceasing the emergency response. This increased the risk that a controller may inappropriately downgrade the emergency response during a developing hypoxic scenario. (Safety issue)
Other finding:
- A 2019 Civil Aviation Safety Authority surveillance event of AGAIR triggered by concerns reported by an AGAIR pilot, including delayed rectification of airworthiness issues, did not include a crosscheck of maintenance releases against the aircraft logbooks, which limited the surveillance team’s ability to determine whether any non-reporting and improper deferral of defects had been taking place at that time.
- The pilot's ability to safely operate the aircraft was almost certainly significantly degraded by the onset of altitude hypoxia.
- While in cruise at flight level 280, both power levers were probably reduced without an appropriate descent rate being initiated, resulting in a progressive reduction of airspeed.
- The aircraft entered a descending anticlockwise turn with an increasing rate of descent. At about 10,500 ft, control input(s) were almost certainly made, probably an attempt to recover, that transitioned the aircraft from a high-speed descent to a spin condition that was likely unrecoverable and which continued until the impact with terrain.
- The pilot had a normalized practice of operating VH-HPY with a cabin altitude that required the use of supplemental oxygen. These flights were conducted without access to a suitable oxygen supply, significantly increasing the risk of altitude hypoxia induced incapacitation.
- The aircraft's pressurization system probably did not attain the required cabin altitude when operating at flight level 280 during the accident flight. The pilot probably knowingly continued the flight with a cabin altitude that required the use of supplemental oxygen, without access to a suitable oxygen supply.
- The AGAIR aircraft VH-HPY pressurization system could not reliably attain the required cabin altitude during flight due to a known, long-term, unresolved intermittent defect. AGAIR management personnel were aware of the defect and, through a combination of inaction, encouragement and, in some instances direct involvement, permitted the aircraft to continue operations at an excessive cabin altitude. (Safety issue)
- AGAIR management exercised ineffective operational control over the line scanning activities. As a result, the ongoing intermittent pressurization defect was not formally recorded, the issues with the aircraft were not communicated to the AGAIR safety manager, and the hazardous practice of operating the aircraft at a cabin altitude that required the use of supplemental oxygen, without access to a suitable oxygen supply, was allowed to continue. (Safety issue)
- The AGAIR head of flying operations did not communicate critical safety information about the known intermittent pressurization defect on VH-HPY when they were phoned by air traffic control about concerns that the pilot may be impacted by hypoxia.
- After being told by the pilot that operations were normal, controllers likely reduced their vigilance about hypoxia and did not re-identify the possibility of hypoxia during the subsequent progressive deterioration of the pilot’s speech.
Other factors that increased risk:
- AGAIR Gulfstream 690 and 695 aircraft were operated with known defects without being recorded on the aircraft’s maintenance releases, likely as a routine practice. For VH-HPY, the absence of documented historical information limited the ability to assess the operational impact of the pressurization defect and the effectiveness of maintenance rectification activities. (Safety issue)
- The Airservices Australia hypoxic pilot emergency checklist did not contain guidance on ceasing the emergency response. This increased the risk that a controller may inappropriately downgrade the emergency response during a developing hypoxic scenario. (Safety issue)
Other finding:
- A 2019 Civil Aviation Safety Authority surveillance event of AGAIR triggered by concerns reported by an AGAIR pilot, including delayed rectification of airworthiness issues, did not include a crosscheck of maintenance releases against the aircraft logbooks, which limited the surveillance team’s ability to determine whether any non-reporting and improper deferral of defects had been taking place at that time.
Final Report: