Crash of a Cessna 340A in Muskogee
Date & Time:
Nov 27, 2024 at 0005 LT
Registration:
N5757C
Survivors:
Yes
Schedule:
Livingston – Muskogee
MSN:
340A-0975
YOM:
1980
Crew on board:
1
Crew fatalities:
Pax on board:
4
Pax fatalities:
Other fatalities:
Total fatalities:
0
Captain / Total hours on type:
245.00
Aircraft flight hours:
3163
Circumstances:
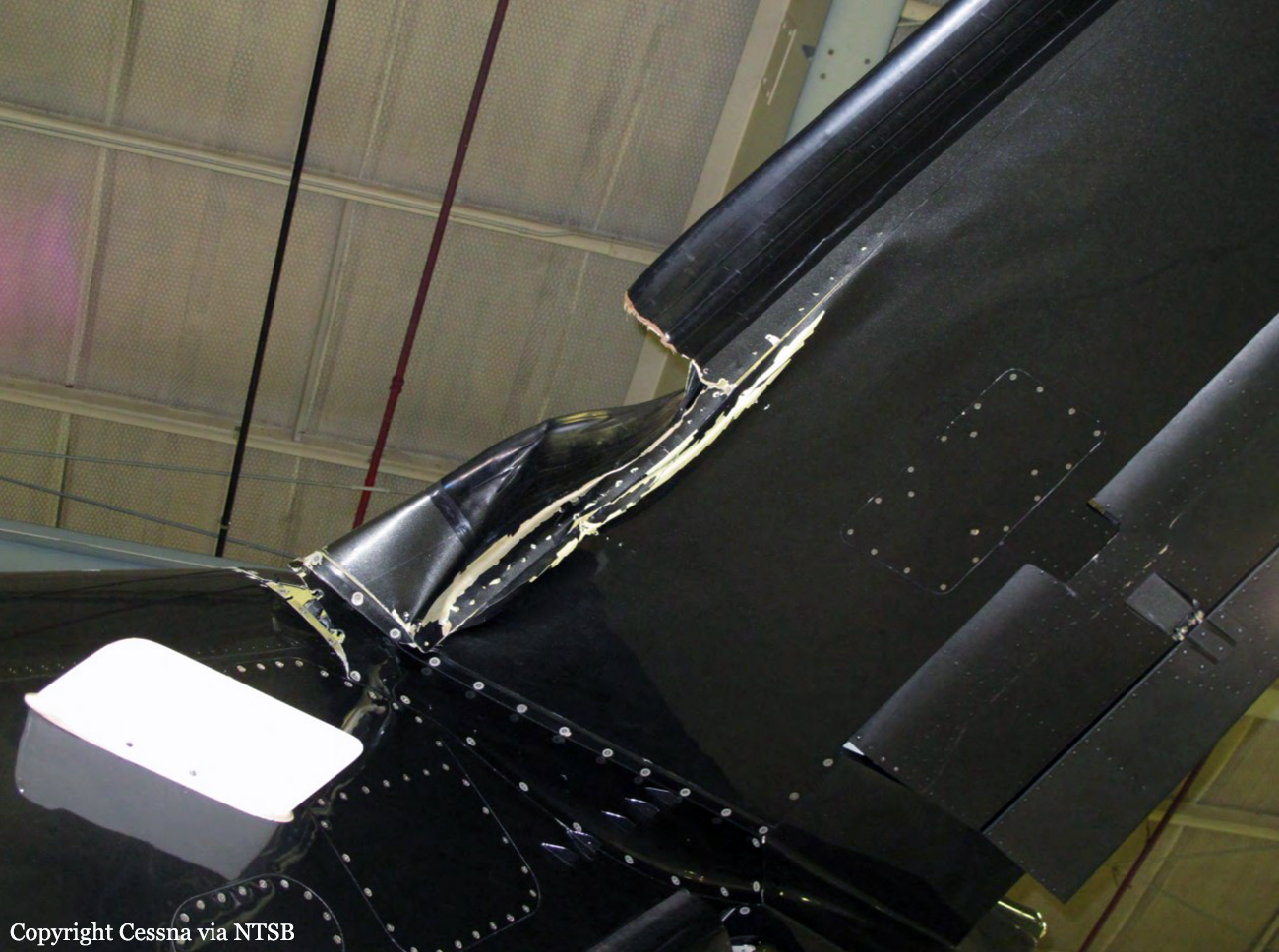
The pilot reported that the airplane was “topped off” with fuel before departing on the night cross-country flight. The pilot performed a preflight inspection, but he did not have his headlamp with him, only his cellular phone. The pilot reported that he typically verified fuel levels at night by feeling inside the fuel tank with his finger, but recalled not verifying the fuel level in the right main fuel tank before departing on the night of the accident flight. The pilot reported that the fuel consumption rate during the first half of the flight was higher than normal due to his operation of the engines slightly rich and his use of the airplane’s heater. While enroute, the pilot transferred fuel from the auxiliary fuel tanks and the left side locker fuel tank to the main fuel tanks. After the “final transfer” was completed, the pilot calculated that there was adequate fuel remaining, including the required reserve fuel, to reach the destination airport; however, he noticed that the indicated fuel remaining levels were less than he expected. Shortly after the pilot was cleared for a visual approach at the destination, the right engine lost total power, followed by the left engine. The pilot reported that, at the time of the initial power loss, gauges indicated that the left side of the airplane had about 30 pounds (about 4.84 gallons) of fuel remaining and the right side had about 30 to 35 pounds (about 4.84 to 5.65 gallons) of fuel remaining. During the subsequent forced landing, the right wing impacted a permanent elevated static display and the airplane came to rest upright on airport property. The airplane sustained substantial damage to the fuselage and the right wing. The pilot and a passenger sustained minor injuries.
Probable cause:
The pilot’s improper fuel planning, which resulted in fuel exhaustion and a total loss of power to both engines.
Final Report: