Crash of a Cessna 414A chancellor in McKinney: 2 killed
Date & Time:
Jun 27, 2024 at 1028 LT
Operator:

Registration:
N414BS
Survivors:
Yes
Schedule:
McKinney - McKinney
MSN:
414A-0504
YOM:
1980
Crew on board:
1
Crew fatalities:
Pax on board:
2
Pax fatalities:
Other fatalities:
Total fatalities:
2
Aircraft flight hours:
7223
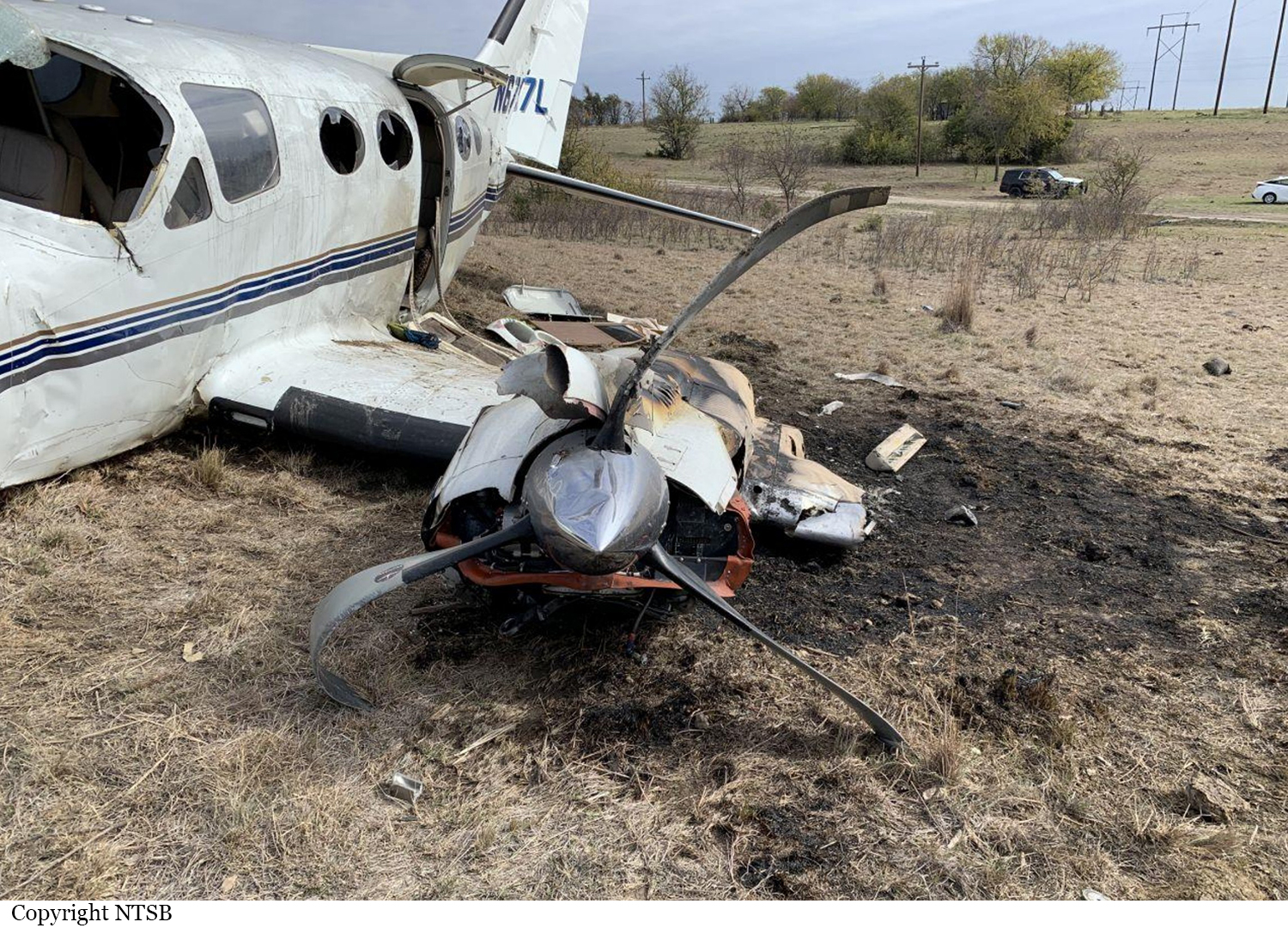
Circumstances:
The pilot was departing on a local flight to check newly installed avionics on the airplane. During takeoff, the airplane lifted off within the performance specifications cited in the airplane flight manual. Shortly after liftoff, the pilot reported to air traffic control (ATC) that he had lost left engine power. The pilot continued the takeoff with the landing gear still extended. A witness stated that the airplane seemed to lose left engine power during the takeoff before reaching taxiway B4, and “yawed left quite a bit.” The remaining runway distance from the B4 taxiway to the departure end of the runway was about 2,600 to 2,700 ft. The witness stated that the airplane was not far past the departure end of runway when it began to turn left. As the pilot continued the takeoff and attempted the climb out, ATC instructed the pilot to turn right. The pilot responded that he was going to turn left, which was a turn into the inoperative engine and in the improper direction due to the greater left rolling tendency and increased likelihood of a loss of control. As the flight progressed, the airplane ground speed slowed to the airplane’s air minimum control speed (Vmc) when it rolled left and impacted terrain in an inverted attitude. The airplane was destroyed. A passenger was injured and two other occupants were killed.
Probable cause:
The pilot's improper decision to attempt continued flight after a loss of left engine power with usable runway remaining and his subsequent failure to follow the emergency procedures and maintain air minimum control speed, which resulted in a loss of control. Contributing to the accident was the pilot's improper fuel tank selection that resulted in a loss of left engine power due to fuel starvation.
Final Report: