Crash of a Beechcraft 200 Super King Air in Elk Grove Village
Date & Time:
Sep 8, 2023 at 1841 LT
Registration:
N220KW
Survivors:
Yes
Schedule:
Chicago – Waterloo
MSN:
BB-1120
YOM:
1983
Crew on board:
1
Crew fatalities:
Pax on board:
0
Pax fatalities:
Other fatalities:
Total fatalities:
0
Captain / Total hours on type:
156.00
Aircraft flight hours:
9817
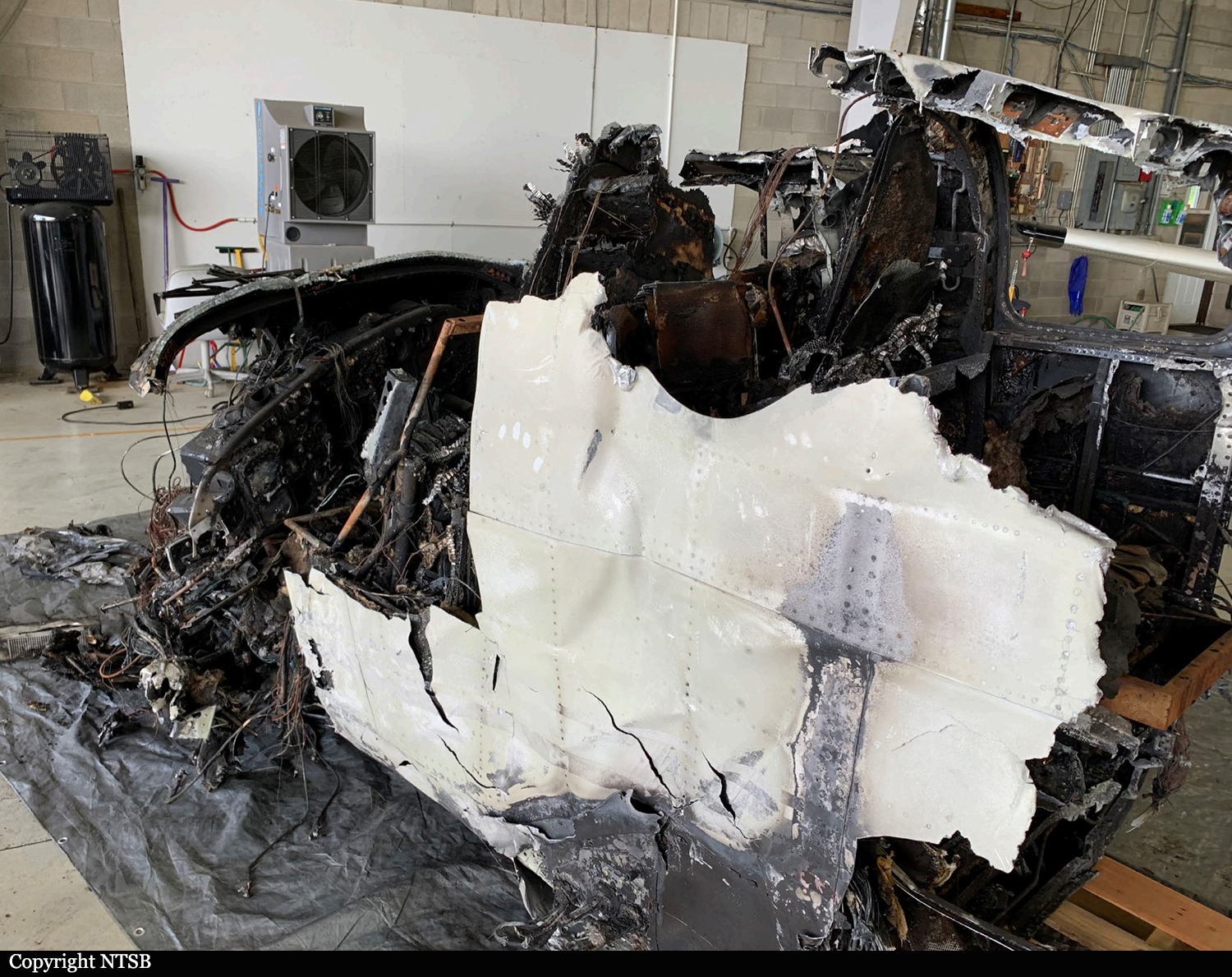
Circumstances:
The pilot reported that he had completed a charter flight and departed to pick up new passengers at an airport about 200 nautical miles away. While on approach to the destination airport, the previous passengers notified the pilot that they were ready to be picked up, so the pilot did not land and turned the airplane back toward the departure airport. The pilot climbed to 10,000 ft and noticed the airplane’s fuel burn was high, so he climbed to 16,000 ft. The pilot reported that “everything was routine until about a 3-mile final” to the runway, when the controller asked the pilot to slow to a final approach speed. An airplane was still on the runway, so the controller told the pilot to go around. The pilot told controllers twice that he had minimum fuel available. The pilot continued on a visual approach for the same runway when the right engine lost power followed by the left engine. He feathered both propellers and made a forced landing to a wooded area. The airplane sustained substantial damage to the fuselage, both wings, and the empennage. The pilot reported that there were no preimpact mechanical malfunctions or failures that would have precluded normal operation. The pilot later stated that he was “trying to do too much with too little” fuel and the accident was a result of poor fuel management. Although the controller directed the pilot to go around, the pilot should have recognized the criticality of the minimum fuel situation and landed the airplane.
Probable cause:
The pilot’s improper fuel planning, that resulted in a total loss of engine power due to fuel exhaustion, and a subsequent forced landing. Also causal was the pilot’s decision to go around with minimum fuel.
Final Report: