Country
Crash of a Boeing 747-412F in Halifax
Date & Time:
Nov 7, 2018 at 0506 LT
Operator:

Registration:
N908AR
Survivors:
Yes
Schedule:
Chicago – Halifax
MSN:
28026/1105
YOM:
1997
Flight number:
KYE4854
Crew on board:
3
Crew fatalities:
Pax on board:
1
Pax fatalities:
Other fatalities:
Total fatalities:
0
Captain / Total hours on type:
166.00
Copilot / Total hours on type:
1239
Aircraft flight hours:
92471
Aircraft flight cycles:
16948
Circumstances:
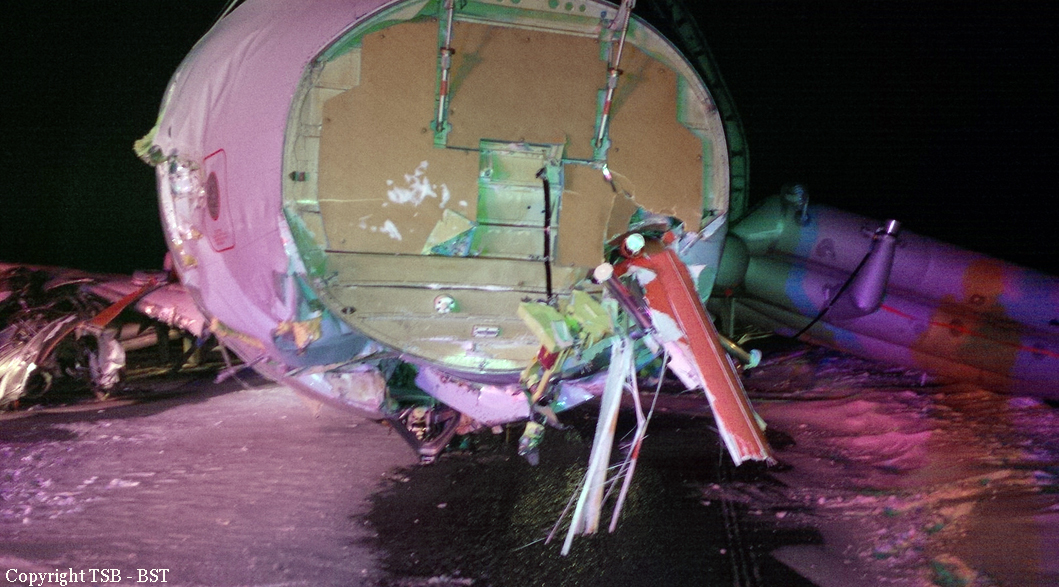
The Sky Lease Cargo Boeing 747-412F aircraft (U.S. registration N908AR, serial number 28026) was conducting flight 4854 (KYE4854) from Chicago/O’Hare International Airport, Illinois, U.S., to Halifax/Stanfield International Airport, Nova Scotia, with 3 crew members, 1 passenger, and no cargo on board. The crew conducted the Runway 14 instrument landing system approach. When the aircraft was 1 minute and 21 seconds from the threshold, the crew realized that there was a tailwind; however, they did not recalculate the performance data to confirm that the landing distance available was still acceptable, likely because of the limited amount of time available before landing. The unexpected tailwind resulted in a greater landing distance required, but this distance did not exceed the length of the runway. The aircraft touched down firmly at approximately 0506 Atlantic Standard Time, during the hours of darkness. After the firm touchdown, for undetermined reasons, the engine No. 1 thrust lever was moved forward of the idle position, causing the speed brakes to retract and the autobrake system to disengage, increasing the distance required to bring the aircraft to a stop. In addition, the right crab angle (4.5°) on initial touchdown, combined with the crosswind component and asymmetric reverser selection, caused the aircraft to deviate to the right of the runway centreline. During the landing roll, the pilot monitoring’s attention was focused on the lateral drift and, as a result, the required callouts regarding the position of the deceleration devices were not made. Although manual brake application began 8 seconds after touchdown, maximum braking effort did not occur until 15 seconds later, when the aircraft was 800 feet from the end of the runway. At this position, it was not possible for the aircraft to stop on the runway and, 5 seconds later, the aircraft departed the end of the runway at a speed of 77 knots and came to a stop 270 m (885 feet) past the end. The aircraft struck the approach light stanchions and the localizer antenna array. The No. 2 engine detached from its pylon during the impact sequence and came to rest under the left horizontal stabilizer, causing a fire in the tail section following the impact. The emergency locator transmitter activated. Aircraft rescue and firefighting personnel responded. All 3 crew members received minor injuries and were taken to the hospital. The passenger was not injured. During the overrun, the aircraft crossed a significant drop of 2.8 m (9 feet) approximately 166 m (544 feet) past the end of the runway and was damaged beyond repair.
Probable cause:
Findings as to causes and contributing factors:
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
1. The ineffective presentation style and sequence of the NOTAMs available to the crew and flight dispatch led them to interpret that Runway 23 was not available for landing at Halifax/Stanfield International Airport.
2. The crew was unaware that the aircraft did not meet the pre-departure landing weight requirements using flaps 25 for Runway 14.
3. Due to the timing of the flight during the nighttime circadian trough and because the crew had had insufficient restorative sleep in the previous 24 hours, the crew was experiencing sleep-related fatigue that degraded their performance and cognitive functioning during the approach and landing.
4. Using unfactored (actual) landing distance charts may have given the crew the impression that landing on Runway 14 would have had a considerable runway safety margin, influencing their decision to continue the landing in the presence of a tailwind.
5. When planning the approach, the crew calculated a faster approach speed of reference speed + 10 knots instead of the recommended reference speed + 5 knots, because they misinterpreted that a wind additive was required for the existing conditions.
6. New information regarding a change of active runway was not communicated by air traffic control directly to the crew, although it was contained within the automatic terminal information service broadcast; as a result, the crew continued to believe that the approach and landing to Runway 14 was the only option available.
7. For the approach, the crew selected the typical flap setting of flaps 25 rather than flaps 30, because they believed they had a sufficient safety margin. This setting increased the landing distance required by 494 feet.
8. The crew were operating in a cognitive context of fatigue and biases that encouraged anchoring to and confirming information that aligned with continuing the initial plan, increasing the likelihood that they would continue the approach.
9. The crew recognized the presence of a tailwind on approach 1 minute and 21 seconds from the threshold; likely due to this limited amount of time, the crew did not recalculate the performance data to confirm that the runway safety margin was still acceptable.
10. An elevated level of stress and workload on short final approach likely exacerbated the performance-impairing effects of fatigue to limit the crew’s ability to determine the effect of the tailwind, influencing their decision to continue the approach.
11. The higher aircraft approach speed, the presence of a tailwind component, and the slight deviation above the glideslope increased the landing distance required to a distance greater than the runway length available.
12. After the firm touchdown, for undetermined reasons, the engine No. 1 thrust lever was moved forward of the idle position, causing the speed brakes to retract and the autobrake system to disengage, increasing the distance required to bring the aircraft to a stop.
13. The right crab angle (4.5°) on initial touchdown, combined with the crosswind component and asymmetric reverser selection, caused the aircraft to deviate to the right of the runway centreline.
14. During the landing roll, the pilot monitoring’s attention was focused on the lateral drift and, as a result, the required callouts regarding the position of the deceleration devices were not made.
15. The pilot flying focused on controlling the lateral deviation and, without the benefit of the landing rollout callouts, did not recognize that all of the deceleration devices were not fully deployed and that the autobrake was disengaged.
16. Although manual brake application began 8 seconds after touchdown, maximum braking effort did not occur until 15 seconds later, when the aircraft was 800 feet from the end of the runway. At this position, it was not possible for the aircraft to stop on the runway and, 5 seconds later, the aircraft departed the end of the runway at a speed of 77 knots and came to a stop 270 m (885 feet) past the end of the runway.
17. During the overrun, the aircraft crossed a significant drop of 2.8 m (9 feet) approximately 166 m (544 feet) past the end of the runway and was damaged beyond repair. While this uneven terrain was beyond the 150 m (492 feet) runway end safety area proposed by Transport Canada, it was within the recommended International Civil Aviation Organization runway end safety area of 300 m (984 feet).
Findings as to risk:
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
1. If the pilot monitoring does not call out approach conditions or approach speed increases, the pilot flying might not make corrections, increasing the risk of a runway overrun.
Other findings:
These items could enhance safety, resolve an issue of controversy, or provide a data point for future safety studies.
1. The investigation concluded that there was no reverted rubber hydroplaning and almost certainly no dynamic hydroplaning during this occurrence.
2. Although viscous hydroplaning can be expected on all wet runways, the investigation found that when maximum braking effort was applied, the aircraft braking was consistent with the expected braking on Runway 14 under the existing wet runway conditions.
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
1. The ineffective presentation style and sequence of the NOTAMs available to the crew and flight dispatch led them to interpret that Runway 23 was not available for landing at Halifax/Stanfield International Airport.
2. The crew was unaware that the aircraft did not meet the pre-departure landing weight requirements using flaps 25 for Runway 14.
3. Due to the timing of the flight during the nighttime circadian trough and because the crew had had insufficient restorative sleep in the previous 24 hours, the crew was experiencing sleep-related fatigue that degraded their performance and cognitive functioning during the approach and landing.
4. Using unfactored (actual) landing distance charts may have given the crew the impression that landing on Runway 14 would have had a considerable runway safety margin, influencing their decision to continue the landing in the presence of a tailwind.
5. When planning the approach, the crew calculated a faster approach speed of reference speed + 10 knots instead of the recommended reference speed + 5 knots, because they misinterpreted that a wind additive was required for the existing conditions.
6. New information regarding a change of active runway was not communicated by air traffic control directly to the crew, although it was contained within the automatic terminal information service broadcast; as a result, the crew continued to believe that the approach and landing to Runway 14 was the only option available.
7. For the approach, the crew selected the typical flap setting of flaps 25 rather than flaps 30, because they believed they had a sufficient safety margin. This setting increased the landing distance required by 494 feet.
8. The crew were operating in a cognitive context of fatigue and biases that encouraged anchoring to and confirming information that aligned with continuing the initial plan, increasing the likelihood that they would continue the approach.
9. The crew recognized the presence of a tailwind on approach 1 minute and 21 seconds from the threshold; likely due to this limited amount of time, the crew did not recalculate the performance data to confirm that the runway safety margin was still acceptable.
10. An elevated level of stress and workload on short final approach likely exacerbated the performance-impairing effects of fatigue to limit the crew’s ability to determine the effect of the tailwind, influencing their decision to continue the approach.
11. The higher aircraft approach speed, the presence of a tailwind component, and the slight deviation above the glideslope increased the landing distance required to a distance greater than the runway length available.
12. After the firm touchdown, for undetermined reasons, the engine No. 1 thrust lever was moved forward of the idle position, causing the speed brakes to retract and the autobrake system to disengage, increasing the distance required to bring the aircraft to a stop.
13. The right crab angle (4.5°) on initial touchdown, combined with the crosswind component and asymmetric reverser selection, caused the aircraft to deviate to the right of the runway centreline.
14. During the landing roll, the pilot monitoring’s attention was focused on the lateral drift and, as a result, the required callouts regarding the position of the deceleration devices were not made.
15. The pilot flying focused on controlling the lateral deviation and, without the benefit of the landing rollout callouts, did not recognize that all of the deceleration devices were not fully deployed and that the autobrake was disengaged.
16. Although manual brake application began 8 seconds after touchdown, maximum braking effort did not occur until 15 seconds later, when the aircraft was 800 feet from the end of the runway. At this position, it was not possible for the aircraft to stop on the runway and, 5 seconds later, the aircraft departed the end of the runway at a speed of 77 knots and came to a stop 270 m (885 feet) past the end of the runway.
17. During the overrun, the aircraft crossed a significant drop of 2.8 m (9 feet) approximately 166 m (544 feet) past the end of the runway and was damaged beyond repair. While this uneven terrain was beyond the 150 m (492 feet) runway end safety area proposed by Transport Canada, it was within the recommended International Civil Aviation Organization runway end safety area of 300 m (984 feet).
Findings as to risk:
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
1. If the pilot monitoring does not call out approach conditions or approach speed increases, the pilot flying might not make corrections, increasing the risk of a runway overrun.
Other findings:
These items could enhance safety, resolve an issue of controversy, or provide a data point for future safety studies.
1. The investigation concluded that there was no reverted rubber hydroplaning and almost certainly no dynamic hydroplaning during this occurrence.
2. Although viscous hydroplaning can be expected on all wet runways, the investigation found that when maximum braking effort was applied, the aircraft braking was consistent with the expected braking on Runway 14 under the existing wet runway conditions.
Final Report:










Crash of a Beechcraft A100 King Air in Margaree
Date & Time:
Aug 16, 2015 at 1616 LT
Operator:

Registration:
C-FDOR
Survivors:
Yes
Schedule:
Halifax – Margaree
MSN:
B-103
YOM:
1972
Crew on board:
2
Crew fatalities:
Pax on board:
2
Pax fatalities:
Other fatalities:
Total fatalities:
0
Captain / Total hours on type:
298.00
Copilot / Total hours on type:
70
Aircraft flight hours:
14345
Circumstances:
On 16 August 2015, a Maritime Air Charter Limited Beechcraft King Air A100 (registration C-FDOR, serial number B-103) was on a charter flight from Halifax Stanfield International Airport, Nova Scotia, to Margaree Aerodrome, Nova Scotia, with 2 pilots and 2 passengers on board. At approximately 1616 Atlantic Daylight Time, while conducting a visual approach to Runway 01, the aircraft touched down hard about 263 feet beyond the threshold. Almost immediately, the right main landing gear collapsed, then the right propeller and wing contacted the runway. The aircraft slid along the runway for about 1350 feet, then veered right and departed off the side of the runway. It came to rest about 1850 feet beyond the threshold and 22 feet from the runway edge. There were no injuries and there was no post-impact fire. The aircraft was substantially damaged. The occurrence took place during daylight hours. The 406-megahertz emergency locator transmitter did not activate.
Probable cause:
Findings:
Findings as to causes and contributing factors:
1. Neither pilot had considered that landing on a short runway at an unfamiliar aerodrome with known high terrain nearby and joining the circuit directly on a left base were hazards that may create additional risks, all of which would increase the crew’s workload.
2. The presence of the tower resulted in the pilot not flying focusing his attention on monitoring the aircraft’s location, rather than on monitoring the flight or the actions of the pilot flying.
3. The crew’s increased workload, together with the unexpected distraction of the presence of the tower, led to a reduced situational awareness that caused them to omit the Landing Checks checklist.
4. At no time during the final descent was the engine power increased above about 400 foot-pounds of torque.
5. Using only pitch to control the rate of descent prevented the pilot flying from precisely controlling the approach, which would have ensured that the flare occurred at the right point and at the right speed.
6. Neither pilot recognized that the steep rate of descent was indicative of an unstable approach.
7. Advancing the propellers to full would have increased the drag and further increased the rate of descent, exacerbating the already unstable approach.
8. The aircraft crossed the runway threshold with insufficient energy to arrest the rate of descent in the landing flare, resulting in a hard landing that caused the right main landing gear to collapse.
Findings as to risk:
1. If data recordings are not available to an investigation, then the identification and communication of safety deficiencies to advance transportation safety may be precluded.
2. If organizations do not use modern safety management practices, then there is an increased risk that hazards will not be identified and risks will not be mitigated.
3. If passenger seats installed in light aircraft are not equipped with shoulder harnesses, then there is an increased risk of passenger injury or death in the event of an accident.
4. If the experience and proficiency of pilots are not factored into crew selection, then there is a risk of suboptimal crew pairing, resulting in a reduction of safety margins.
5. If pilots do not carry out checklists in accordance with the company’s and manufacturer’s instructions, then there is a risk that a critical item may be missed, which could jeopardize the safety of the flight.
6. If crew resource management is not used and continuously fostered, then there is a risk that pilots will be unprepared to avoid or mitigate crew errors encountered during flight.
7. If organizations do not have a clearly defined go-around policy, then there is a risk that flight crews will continue an unstable approach, increasing the risk of an approach-and-landing accident.
8. If pilots are not prepared to conduct a go-around on every approach, then there is a risk that they may not respond to situations that require a go-around.
9. If operators do not have a stable approach policy, then there is a risk that an unstable approach will be continued to a landing, increasing the risk of an approach-andlanding accident.
10. If an organization’s safety culture does not fully promote the goals of a safety management system, then it is unlikely that it will be effective in reducing risk.
Other findings:
1. There were insufficient forward impact forces to automatically activate the emergency locator transmitter.
Findings as to causes and contributing factors:
1. Neither pilot had considered that landing on a short runway at an unfamiliar aerodrome with known high terrain nearby and joining the circuit directly on a left base were hazards that may create additional risks, all of which would increase the crew’s workload.
2. The presence of the tower resulted in the pilot not flying focusing his attention on monitoring the aircraft’s location, rather than on monitoring the flight or the actions of the pilot flying.
3. The crew’s increased workload, together with the unexpected distraction of the presence of the tower, led to a reduced situational awareness that caused them to omit the Landing Checks checklist.
4. At no time during the final descent was the engine power increased above about 400 foot-pounds of torque.
5. Using only pitch to control the rate of descent prevented the pilot flying from precisely controlling the approach, which would have ensured that the flare occurred at the right point and at the right speed.
6. Neither pilot recognized that the steep rate of descent was indicative of an unstable approach.
7. Advancing the propellers to full would have increased the drag and further increased the rate of descent, exacerbating the already unstable approach.
8. The aircraft crossed the runway threshold with insufficient energy to arrest the rate of descent in the landing flare, resulting in a hard landing that caused the right main landing gear to collapse.
Findings as to risk:
1. If data recordings are not available to an investigation, then the identification and communication of safety deficiencies to advance transportation safety may be precluded.
2. If organizations do not use modern safety management practices, then there is an increased risk that hazards will not be identified and risks will not be mitigated.
3. If passenger seats installed in light aircraft are not equipped with shoulder harnesses, then there is an increased risk of passenger injury or death in the event of an accident.
4. If the experience and proficiency of pilots are not factored into crew selection, then there is a risk of suboptimal crew pairing, resulting in a reduction of safety margins.
5. If pilots do not carry out checklists in accordance with the company’s and manufacturer’s instructions, then there is a risk that a critical item may be missed, which could jeopardize the safety of the flight.
6. If crew resource management is not used and continuously fostered, then there is a risk that pilots will be unprepared to avoid or mitigate crew errors encountered during flight.
7. If organizations do not have a clearly defined go-around policy, then there is a risk that flight crews will continue an unstable approach, increasing the risk of an approach-and-landing accident.
8. If pilots are not prepared to conduct a go-around on every approach, then there is a risk that they may not respond to situations that require a go-around.
9. If operators do not have a stable approach policy, then there is a risk that an unstable approach will be continued to a landing, increasing the risk of an approach-andlanding accident.
10. If an organization’s safety culture does not fully promote the goals of a safety management system, then it is unlikely that it will be effective in reducing risk.
Other findings:
1. There were insufficient forward impact forces to automatically activate the emergency locator transmitter.
Final Report:


Crash of an Airbus A320-211 in Halifax
Date & Time:
Mar 29, 2015 at 0030 LT
Operator:

Registration:
C-FTJP
Survivors:
Yes
Schedule:
Toronto – Halifax
MSN:
233
YOM:
1991
Flight number:
AC624
Crew on board:
5
Crew fatalities:
Pax on board:
133
Pax fatalities:
Other fatalities:
Total fatalities:
0
Captain / Total hours on type:
5755.00
Copilot / Total hours on type:
6392
Aircraft flight hours:
75103
Circumstances:
On 29 March 2015, an Air Canada Airbus Industrie A320-211 (registration C-FTJP, serial number 233), operating as Air Canada flight 624, was on a scheduled flight from Toronto/Lester B. Pearson International Airport, Ontario, to Halifax/Stanfield International Airport, Nova Scotia, with 133 passengers and 5 crew members on board. At approximately 0030 Atlantic Daylight Time, while conducting a non-precision approach to Runway 05, the aircraft severed power lines, then struck the snow-covered ground about 740 feet before the runway threshold. The aircraft continued airborne through the localizer antenna array, then struck the ground twice more before sliding along the runway. It came to rest on the left side of the runway, about 1900 feet beyond the threshold. The aircraft was evacuated; 25 people sustained injuries and were taken to local hospitals. The aircraft was destroyed. There was no post-impact fire. The emergency locator transmitter was not activated. The accident occurred during the hours of darkness.
Probable cause:
Findings as to causes and contributing factors:
1. Air Canada’s standard operating procedure (SOP) and practice when flying in flight path angle guidance mode was that, once the aircraft was past the final approach fix, the flight crews were not required to monitor the aircraft’s altitude and distance from the threshold or to make any adjustments to the flight path angle. This practice was not in accordance with the flight crew operating manuals of Air Canada or Airbus.
2. As per Air Canada’s practice, once the flight path angle was selected and the aircraft began to descend, the flight crew did not monitor the altitude and distance from the threshold, nor did they make any adjustments to the flight path angle.
3. The flight crew did not notice that the aircraft had drifted below and diverged from the planned vertical descent angle flight profile, nor were they aware that the aircraft had crossed the minimum descent altitude further back from the threshold.
4. Considering the challenging conditions to acquire and maintain the visual cues, it is likely the flight crew delayed disconnecting the autopilot until beyond the minimum descent altitude because of their reliance on the autopilot system.
5. The approach and runway lights were not changed from setting 4 to setting 5; therefore, these lights were not at their maximum brightness setting during the approach.
6. The system to control the airfield lighting’s preset selections for brightness setting 4 was not in accordance with the NAV CANADA Air Traffic Control Manual of Operations requirement for the omnidirectional approach lighting system to be at its brightest settings.
7. The limited number of visual cues and the short time that they were available to the flight crew, combined with potential visual illusions and the reduced brightness of the approach and runway lights, diminished the flight crew’s ability to detect that the aircraft’s approach path was taking it short of the runway.
8. The flight crew’s recognition that the aircraft was too low during the approach would have been delayed because of plan continuation bias.
9. The aircraft struck terrain approximately 740 feet short of the runway threshold, bounced twice, and then slid along the runway before coming to a rest approximately 1900 feet beyond the runway threshold.
10. At some time during the impact sequence, the captain’s head struck the glare shield because there were insufficient acceleration forces to lock the shoulder harness and prevent movement of his upper body.
11. The first officer sustained a head injury and serious injury to the right eye as a result of striking the glare shield because the automatic locking feature of the right-side shoulder-harness inertia reel was unserviceable.
12. A flight attendant was injured by a coffee brewer that came free of its mounting base because its locking system was not correctly engaged.
13. Because no emergency was expected, the passengers and cabin crew were not in a brace position at the time of the initial impact.
14. Most of the injuries sustained by the passengers were consistent with not adopting a brace position.
Findings as to risk:
1. If aircraft cockpit voice recorder installations do not have an independent power supply, additional, potentially valuable information will not be available for an investigation.
2. If Transport Canada does not consistently follow its protocol for the assessment of aeromedical risk and ongoing surveillance in applicants who suffer from obstructive sleep apnea, some of the safety benefit of medical examinations will be lost, increasing the risk that pilots will fly with a medical condition that poses a risk to safety.
3. If new regulations on the use of child-restraint systems are not implemented, lap-held infants and young children are exposed to undue risk and are not provided with a level of safety equivalent to that for adult passengers.
4. If passengers do not dress appropriately for safe travel, they risk being unprepared for adverse weather conditions during an emergency evacuation.
5. If the type of approach lighting system on a runway is not factored into the minimum visibility required to carry out an approach, in conditions of reduced visibility, the lighting available risks being less than adequate for flight crews to assess the aircraft’s position and decide whether or not to continue the approach to a safe landing.
6. If they do not incorporate a means of absorbing forces along their longitudinal axis, vertically mounted, non-structural beams (channels, tubes, etc.) in cargo compartments could penetrate the cabin floor when the fuselage strikes the water or ground, increasing the risk of aircraft occupants being injured or emergency egress being impaired.
7. If an aircraft manufacturer’s maintenance instructions do not include the component manufacturer’s safety-critical test criteria, the component risks not being maintained in an airworthy condition.
8. If there is a complete loss of electrical and battery power and the passenger address system does not have an independent emergency power supply, the passenger address system will be inoperable, and the initial command to evacuate or to convey other emergency instructions may be delayed, putting the safety of passengers and crew at risk.
9. If passengers retrieve or attempt to retrieve their carry-on baggage during an evacuation, they are putting themselves and other passengers at a greater risk of injury or death.
10. If passengers do not pay attention to the pre-departure safety briefings or review the safety-features cards, they may be unprepared to react appropriately in an accident, increasing their risk of injury or death.
11. If an organization’s emergency response plan does not identify all available transportation resources, there is an increased risk that evacuated passengers and crew will not be moved from an accident site in a timely manner.
12. If organizations do not practise transporting persons from an on-airport accident site, they may be insufficiently prepared to react appropriately to an actual accident, which may increase the time required to evacuate the passengers and crew.
Other findings:
1. The service director assessed the evacuation flow as good and determined that there was therefore no need to open the R1 door.
2. The flight attendants stationed in the rear of the aircraft noted no life-threatening hazards. Because no evacuation order had been given, and deplaned passengers and firefighters were observed walking near the rear of the aircraft in an area where the deployment of the rear slides may have created additional hazards or risks, the flight attendants determined that there was no requirement to open the L2 and R2 doors.
3. Although Transport Canada required the dual-exit drill to be implemented in training, it did not require all cabin crew to receive the training before an organization implemented the 1:50 ratio.
4. At the time of the accident, neither the service director nor the flight attendants had received the dual-exit training, nor were they aware of the requirement for such training in order for Air Canada to operate with the exemption allowing 1 flight attendant for each unit of 50 passengers.
5. Although Transport Canada had reviewed and approved Air Canada’s aircraft operating manual and the standard operating procedures (SOPs), it had not identified the discrepancy between the Air Canada SOPs and the Airbus flight crew operating manual regarding the requirement to monitor the aircraft’s vertical flight path beyond the final approach fix when the flight path angle guidance mode is engaged.
6. A discrepancy in the Halifax International Airport Authority’s standby generators’ control circuitry caused the 2 standby generators to stop producing power.
7. Air Canada’s emergency response plan for Halifax/Stanfield International Airport indicated that the airline was responsible for the transportation of passengers from an accident site.
8. Air Canada’s emergency response plan did not identify the airport’s Park’N Fly minibuses as transportation resources. 9. The Halifax International Airport Authority’s emergency response plan did not identify that the airport Park’N Fly mini-buses could be used to transport the uninjured passengers, nor did it provide instructions on when and how to request and dispatch any transportation resources available at the airport.
10. The Air Canada Flight Operations Manual did not identify that the required visual reference should enable the pilot to assess aircraft position and rate of change of position in order to continue the approach to a landing.
11. In Canada, the minimum visibility that is authorized by the operations specification for non-precision approaches does not take into account the type of approach lighting system installed on the runway.
12. It is likely that, during the emergency, a passenger activated the L1 door gust lock release pushbutton while trying to expedite his or her exit, which allowed the door to move freely.
13. The passenger seatbacks were dislodged because the shear pins had sheared, likely as a result of contact with passengers during the impact sequence or emergency egress.
14. Recovery of the uninjured passengers from the accident site was delayed owing to a number of factors, including the severe weather conditions; the failure of the airport’s 2 standby generators to provide backup power after the loss of utility power; the loss of the airport operations radio network; and the lack of arrangements for the dispatch of transportation vehicles until after emergency response services had advised that all passengers were evacuated and the site was all clear.
15. Given that the captain rarely used continuous positive airway pressure therapy, he would have been at risk of experiencing fatigue related to chronic sleep disruption caused by obstructive sleep apnea. However, there was no indication that fatigue played a causal or contributory role in this occurrence.
1. Air Canada’s standard operating procedure (SOP) and practice when flying in flight path angle guidance mode was that, once the aircraft was past the final approach fix, the flight crews were not required to monitor the aircraft’s altitude and distance from the threshold or to make any adjustments to the flight path angle. This practice was not in accordance with the flight crew operating manuals of Air Canada or Airbus.
2. As per Air Canada’s practice, once the flight path angle was selected and the aircraft began to descend, the flight crew did not monitor the altitude and distance from the threshold, nor did they make any adjustments to the flight path angle.
3. The flight crew did not notice that the aircraft had drifted below and diverged from the planned vertical descent angle flight profile, nor were they aware that the aircraft had crossed the minimum descent altitude further back from the threshold.
4. Considering the challenging conditions to acquire and maintain the visual cues, it is likely the flight crew delayed disconnecting the autopilot until beyond the minimum descent altitude because of their reliance on the autopilot system.
5. The approach and runway lights were not changed from setting 4 to setting 5; therefore, these lights were not at their maximum brightness setting during the approach.
6. The system to control the airfield lighting’s preset selections for brightness setting 4 was not in accordance with the NAV CANADA Air Traffic Control Manual of Operations requirement for the omnidirectional approach lighting system to be at its brightest settings.
7. The limited number of visual cues and the short time that they were available to the flight crew, combined with potential visual illusions and the reduced brightness of the approach and runway lights, diminished the flight crew’s ability to detect that the aircraft’s approach path was taking it short of the runway.
8. The flight crew’s recognition that the aircraft was too low during the approach would have been delayed because of plan continuation bias.
9. The aircraft struck terrain approximately 740 feet short of the runway threshold, bounced twice, and then slid along the runway before coming to a rest approximately 1900 feet beyond the runway threshold.
10. At some time during the impact sequence, the captain’s head struck the glare shield because there were insufficient acceleration forces to lock the shoulder harness and prevent movement of his upper body.
11. The first officer sustained a head injury and serious injury to the right eye as a result of striking the glare shield because the automatic locking feature of the right-side shoulder-harness inertia reel was unserviceable.
12. A flight attendant was injured by a coffee brewer that came free of its mounting base because its locking system was not correctly engaged.
13. Because no emergency was expected, the passengers and cabin crew were not in a brace position at the time of the initial impact.
14. Most of the injuries sustained by the passengers were consistent with not adopting a brace position.
Findings as to risk:
1. If aircraft cockpit voice recorder installations do not have an independent power supply, additional, potentially valuable information will not be available for an investigation.
2. If Transport Canada does not consistently follow its protocol for the assessment of aeromedical risk and ongoing surveillance in applicants who suffer from obstructive sleep apnea, some of the safety benefit of medical examinations will be lost, increasing the risk that pilots will fly with a medical condition that poses a risk to safety.
3. If new regulations on the use of child-restraint systems are not implemented, lap-held infants and young children are exposed to undue risk and are not provided with a level of safety equivalent to that for adult passengers.
4. If passengers do not dress appropriately for safe travel, they risk being unprepared for adverse weather conditions during an emergency evacuation.
5. If the type of approach lighting system on a runway is not factored into the minimum visibility required to carry out an approach, in conditions of reduced visibility, the lighting available risks being less than adequate for flight crews to assess the aircraft’s position and decide whether or not to continue the approach to a safe landing.
6. If they do not incorporate a means of absorbing forces along their longitudinal axis, vertically mounted, non-structural beams (channels, tubes, etc.) in cargo compartments could penetrate the cabin floor when the fuselage strikes the water or ground, increasing the risk of aircraft occupants being injured or emergency egress being impaired.
7. If an aircraft manufacturer’s maintenance instructions do not include the component manufacturer’s safety-critical test criteria, the component risks not being maintained in an airworthy condition.
8. If there is a complete loss of electrical and battery power and the passenger address system does not have an independent emergency power supply, the passenger address system will be inoperable, and the initial command to evacuate or to convey other emergency instructions may be delayed, putting the safety of passengers and crew at risk.
9. If passengers retrieve or attempt to retrieve their carry-on baggage during an evacuation, they are putting themselves and other passengers at a greater risk of injury or death.
10. If passengers do not pay attention to the pre-departure safety briefings or review the safety-features cards, they may be unprepared to react appropriately in an accident, increasing their risk of injury or death.
11. If an organization’s emergency response plan does not identify all available transportation resources, there is an increased risk that evacuated passengers and crew will not be moved from an accident site in a timely manner.
12. If organizations do not practise transporting persons from an on-airport accident site, they may be insufficiently prepared to react appropriately to an actual accident, which may increase the time required to evacuate the passengers and crew.
Other findings:
1. The service director assessed the evacuation flow as good and determined that there was therefore no need to open the R1 door.
2. The flight attendants stationed in the rear of the aircraft noted no life-threatening hazards. Because no evacuation order had been given, and deplaned passengers and firefighters were observed walking near the rear of the aircraft in an area where the deployment of the rear slides may have created additional hazards or risks, the flight attendants determined that there was no requirement to open the L2 and R2 doors.
3. Although Transport Canada required the dual-exit drill to be implemented in training, it did not require all cabin crew to receive the training before an organization implemented the 1:50 ratio.
4. At the time of the accident, neither the service director nor the flight attendants had received the dual-exit training, nor were they aware of the requirement for such training in order for Air Canada to operate with the exemption allowing 1 flight attendant for each unit of 50 passengers.
5. Although Transport Canada had reviewed and approved Air Canada’s aircraft operating manual and the standard operating procedures (SOPs), it had not identified the discrepancy between the Air Canada SOPs and the Airbus flight crew operating manual regarding the requirement to monitor the aircraft’s vertical flight path beyond the final approach fix when the flight path angle guidance mode is engaged.
6. A discrepancy in the Halifax International Airport Authority’s standby generators’ control circuitry caused the 2 standby generators to stop producing power.
7. Air Canada’s emergency response plan for Halifax/Stanfield International Airport indicated that the airline was responsible for the transportation of passengers from an accident site.
8. Air Canada’s emergency response plan did not identify the airport’s Park’N Fly minibuses as transportation resources. 9. The Halifax International Airport Authority’s emergency response plan did not identify that the airport Park’N Fly mini-buses could be used to transport the uninjured passengers, nor did it provide instructions on when and how to request and dispatch any transportation resources available at the airport.
10. The Air Canada Flight Operations Manual did not identify that the required visual reference should enable the pilot to assess aircraft position and rate of change of position in order to continue the approach to a landing.
11. In Canada, the minimum visibility that is authorized by the operations specification for non-precision approaches does not take into account the type of approach lighting system installed on the runway.
12. It is likely that, during the emergency, a passenger activated the L1 door gust lock release pushbutton while trying to expedite his or her exit, which allowed the door to move freely.
13. The passenger seatbacks were dislodged because the shear pins had sheared, likely as a result of contact with passengers during the impact sequence or emergency egress.
14. Recovery of the uninjured passengers from the accident site was delayed owing to a number of factors, including the severe weather conditions; the failure of the airport’s 2 standby generators to provide backup power after the loss of utility power; the loss of the airport operations radio network; and the lack of arrangements for the dispatch of transportation vehicles until after emergency response services had advised that all passengers were evacuated and the site was all clear.
15. Given that the captain rarely used continuous positive airway pressure therapy, he would have been at risk of experiencing fatigue related to chronic sleep disruption caused by obstructive sleep apnea. However, there was no indication that fatigue played a causal or contributory role in this occurrence.
Final Report:




















Crash of a Cessna 414A Chancellor off Sydney: 2 killed
Date & Time:
Aug 5, 2010 at 2337 LT
Operator:

Registration:
C-GENG
Survivors:
No
Schedule:
Butonville - Sydney
MSN:
414A-0288
YOM:
1979
Crew on board:
1
Crew fatalities:
Pax on board:
1
Pax fatalities:
Other fatalities:
Total fatalities:
2
Aircraft flight hours:
9677
Circumstances:
The privately owned Cessna 414A departed Toronto/Buttonville Municipal Airport, Ontario, en route to Sydney, Nova Scotia. The flight was operating under an instrument flight rules flight plan with the pilot-in-command and the aircraft owner on board. Nearing Sydney, the aircraft was cleared to conduct an instrument approach. At the final approach waypoint the pilot was advised to discontinue the approach due to conflicting traffic. While manoeuvring for a second approach, the aircraft departed from controlled flight, entered a rapid descent and impacted the water at 2335 Atlantic Daylight Time. The aircraft wreckage was located using a side-scan sonar 11 days later, in 170 feet of water. The aircraft had been destroyed and both occupants were fatally injured. No signal was detected from the emergency locator transmitter.
Probable cause:
Findings as to Causes and Contributing Factors:
1. It is likely that the PIC and the owner were both suffering some degree of spatial disorientation during the final portion of the flight. This resulted in a loss of control of the aircraft and the crew was unable to recover prior to contacting the surface of the water.
2. The PIC did not accept assistance in the form of radar vectors, which contributed to the workload during the approach.
3. Self-imposed pressure likely influenced the crew’s decision to depart Buttonville despite the flight conditions, lengthy day, and lack of experience with the aircraft and the destination airport.
Other Findings:
1. It could not be conclusively determined who was flying the aircraft at the time of the occurrence.
2. The lack of onboard recording devices prevented the investigation from determining the reasons why the aircraft departed controlled flight.
3. The practice of placing aircraft technical records on board aircraft may impede an investigation if the records are lost due to an accident.
1. It is likely that the PIC and the owner were both suffering some degree of spatial disorientation during the final portion of the flight. This resulted in a loss of control of the aircraft and the crew was unable to recover prior to contacting the surface of the water.
2. The PIC did not accept assistance in the form of radar vectors, which contributed to the workload during the approach.
3. Self-imposed pressure likely influenced the crew’s decision to depart Buttonville despite the flight conditions, lengthy day, and lack of experience with the aircraft and the destination airport.
Other Findings:
1. It could not be conclusively determined who was flying the aircraft at the time of the occurrence.
2. The lack of onboard recording devices prevented the investigation from determining the reasons why the aircraft departed controlled flight.
3. The practice of placing aircraft technical records on board aircraft may impede an investigation if the records are lost due to an accident.
Final Report:

Crash of a Bombardier BD-700-1A11 Global Express 5000 in Fox Harbour
Date & Time:
Nov 11, 2007 at 1434 LT
Operator:

Registration:
C-GXPR
Survivors:
Yes
Schedule:
Hamilton – Fox Harbour
MSN:
9211
YOM:
2006
Crew on board:
2
Crew fatalities:
Pax on board:
8
Pax fatalities:
Other fatalities:
Total fatalities:
0
Captain / Total hours on type:
64.00
Copilot / Total hours on type:
9
Aircraft flight hours:
92
Aircraft flight cycles:
26
Circumstances:
The aircraft, operated by Jetport Inc., departed Hamilton, Ontario, for Fox Harbour, Nova Scotia, with two crew members and eight passengers on board. At approximately 1434 Atlantic standard time, the aircraft touched down seven feet short of Runway 33 at the Fox Harbour aerodrome. The main landing gear was damaged when it struck the edge of the runway, and directional control was lost when the right main landing gear collapsed. The aircraft departed the right side of the runway and came to a stop 1000 feet from the initial touchdown point. All occupants evacuated the aircraft. One crew member and one passenger suffered serious injuries; the other eight occupants suffered minor injuries. The aircraft sustained major structural damage.
Probable cause:
Findings as to Risk:
1. Because aircraft EWH information is not readily available to pilots, crews may continue to conduct approaches with an aircraft mismatched to the visual glide slope indicator (VGSI) system, increasing the risk of a reduced TCH safety margin.
2. Due to limited knowledge of the various VGSI systems in operation and their limitations, flight crews will continue to follow visual guidance that might not provide for safe TCH.
3. Jetport did not develop an accurate company risk profile. This precluded identification of systemic safety deficiencies and development of appropriate mitigation strategies.
4. If adequate safety oversight of POC operators is not maintained by the regulator, or the delegated organization, especially during SMS implementation, there is an increased risk that safety deficiencies will not be identified.
5. The fact that the Canadian Business Aviation Association (CBAA) did not insist that milestones for SMS implementation and development be followed may result in some POC operators never reaching full SMS compliance.
6. If Transport Canada does not ensure that the CBAA fulfills its responsibilities for adequate oversight of the Canadian Aviation Regulations (CARs) subpart 604 community, safety deficiencies will not be identified and addressed.
7. The audit of Jetport’s SMS, conducted by the CBAA–accredited auditor, did not identify the deficiencies in the program or make any suggestions for improvement. Without a comprehensive audit of an operator’s SMS, deficiencies could exist resulting in the operator’s inability to implement an effective mitigation strategy.
8. Contrary to the recommendations made in the Transport Canada/CBAA feasibility studies, the CBAA did not have a quality assurance program for its audit process. As a result, there is a risk that the CBAA will fail to identify weaknesses in the POC audit program.
9. At the time of the accident, no one at Fox Harbour (CFH4) had been assigned responsibility for regular maintenance of the APAPI, therefore preventing timely identification of APAPI equipment misalignment.
10. Jetport’s risk analysis before the introduction of the Global 5000 did not identify the incompatibility between the EWH of the aircraft and the APAPI at CFH4.
11. Not wearing shoulder harnesses during landings and take-offs increases the potential risk of passenger injuries.
12. Passengers not wearing footwear could impede evacuation, increase the risk of injury, and reduce post-crash mobility and (potentially) survival.
Other Findings:
1. A SMS integrates sound risk management policies, practices, and procedures into day-to-day operations and, properly implemented, offers great potential to reduce accidents.
2. Contrary to its own assessment protocol, Transport Canada did not document its decision to close off the CBAA assessment even though the CBAA had not submitted an acceptable corrective action plan.
3. Depiction of the different types of VGSIs differs, depending on the publication.
1. Because aircraft EWH information is not readily available to pilots, crews may continue to conduct approaches with an aircraft mismatched to the visual glide slope indicator (VGSI) system, increasing the risk of a reduced TCH safety margin.
2. Due to limited knowledge of the various VGSI systems in operation and their limitations, flight crews will continue to follow visual guidance that might not provide for safe TCH.
3. Jetport did not develop an accurate company risk profile. This precluded identification of systemic safety deficiencies and development of appropriate mitigation strategies.
4. If adequate safety oversight of POC operators is not maintained by the regulator, or the delegated organization, especially during SMS implementation, there is an increased risk that safety deficiencies will not be identified.
5. The fact that the Canadian Business Aviation Association (CBAA) did not insist that milestones for SMS implementation and development be followed may result in some POC operators never reaching full SMS compliance.
6. If Transport Canada does not ensure that the CBAA fulfills its responsibilities for adequate oversight of the Canadian Aviation Regulations (CARs) subpart 604 community, safety deficiencies will not be identified and addressed.
7. The audit of Jetport’s SMS, conducted by the CBAA–accredited auditor, did not identify the deficiencies in the program or make any suggestions for improvement. Without a comprehensive audit of an operator’s SMS, deficiencies could exist resulting in the operator’s inability to implement an effective mitigation strategy.
8. Contrary to the recommendations made in the Transport Canada/CBAA feasibility studies, the CBAA did not have a quality assurance program for its audit process. As a result, there is a risk that the CBAA will fail to identify weaknesses in the POC audit program.
9. At the time of the accident, no one at Fox Harbour (CFH4) had been assigned responsibility for regular maintenance of the APAPI, therefore preventing timely identification of APAPI equipment misalignment.
10. Jetport’s risk analysis before the introduction of the Global 5000 did not identify the incompatibility between the EWH of the aircraft and the APAPI at CFH4.
11. Not wearing shoulder harnesses during landings and take-offs increases the potential risk of passenger injuries.
12. Passengers not wearing footwear could impede evacuation, increase the risk of injury, and reduce post-crash mobility and (potentially) survival.
Other Findings:
1. A SMS integrates sound risk management policies, practices, and procedures into day-to-day operations and, properly implemented, offers great potential to reduce accidents.
2. Contrary to its own assessment protocol, Transport Canada did not document its decision to close off the CBAA assessment even though the CBAA had not submitted an acceptable corrective action plan.
3. Depiction of the different types of VGSIs differs, depending on the publication.
Final Report:


