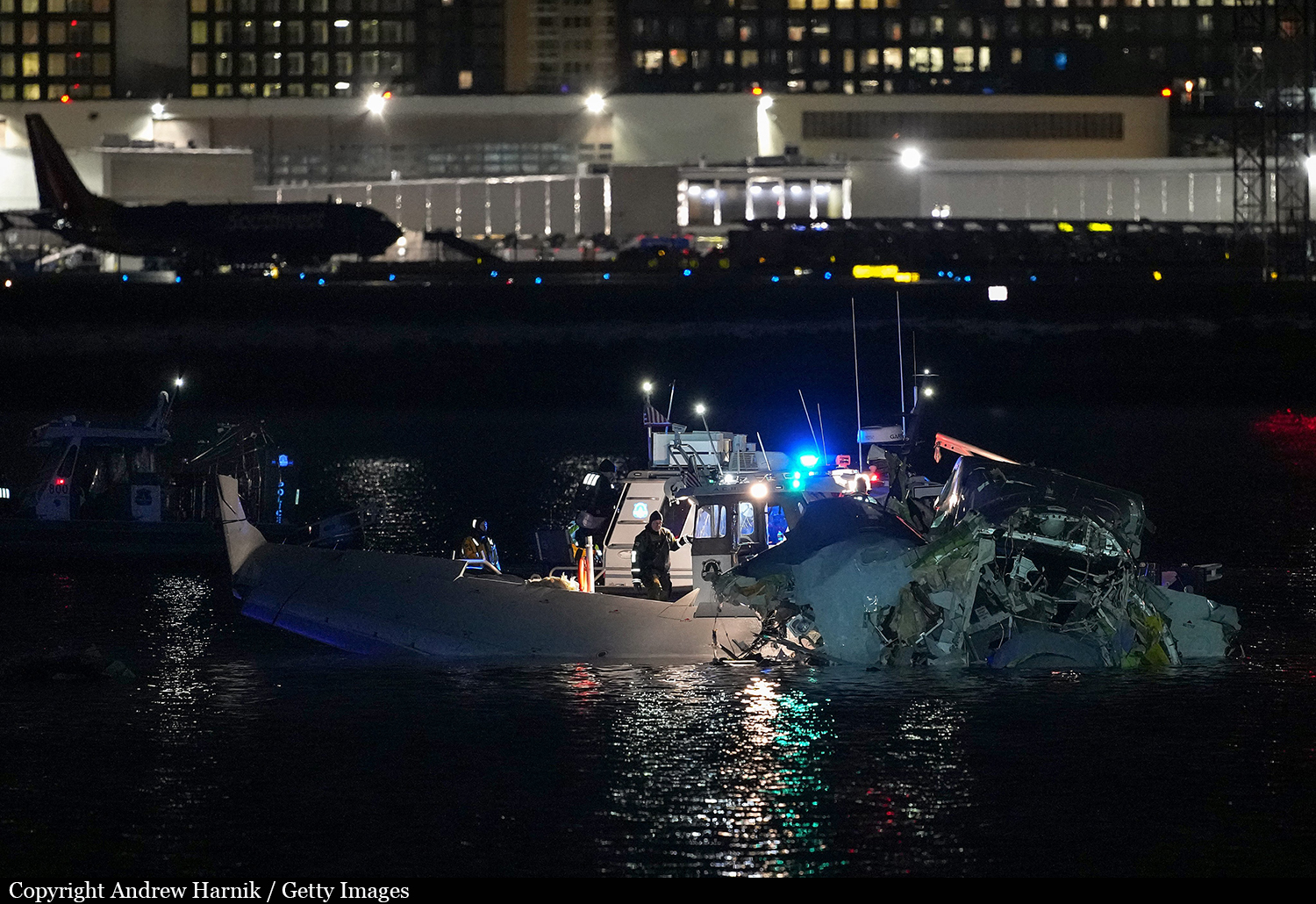
Crash of a Canadair CRJ-701ER in Washington DC: 64 killed
Date & Time:
Jan 29, 2025 at 2048 LT
Operator:

Registration:
N709PS
Survivors:
No
Schedule:
Wichita - Washington DC
MSN:
10165
YOM:
2004
Flight number:
AA5342
Crew on board:
4
Crew fatalities:
Pax on board:
60
Pax fatalities:
Other fatalities:
Total fatalities:
64
Captain / Total hours on type:
3024.00
Copilot / Total hours on type:
965
Circumstances:
On January 29, 2025, about 2048 eastern standard time (EST), a Sikorsky UH-60L, operated by the US Army under the callsign PAT25 (Priority Air Transport Flight 25), and an MHI (Mitsubishi Heavy Industries) RJ Aviation (formerly Bombardier) CL-600-2C10 (CRJ700), N709PS, operated by PSA Airlines as American Airlines flight 5342, collided in flight about 0.5 miles southeast of Ronald Reagan Washington National Airport (DCA), Arlington, Virginia, and impacted the Potomac River in southwest Washington, DC. The 2 pilots, 2 flight attendants, and 60 passengers on board the airplane and all 3 crew members on board the helicopter died. Both aircraft were destroyed as a result of the accident. Flight 5342 was operating under the provisions of Title 14 Code of Federal Regulations Part 121 as a scheduled domestic passenger flight from Wichita Dwight D. Eisenhower National Airport, Wichita, Kansas, to DCA. PAT25 originated from Davison Army Airfield (DAA), Fort Belvoir, Virginia, for the purpose of the pilot’s annual standardization evaluation flight with the use of night vision goggles (NVGs). Night visual meteorological conditions prevailed in the area of DCA at the time of the accident. PAT25 departed DAA and landed at sites in Virginia and Maryland before the crew turned south toward Washington, DC, and was cleared by the DCA tower controller (who was working combined local control and helicopter control positions) to transition the DCA airspace via helicopter Routes 1 and 4 before proceeding back to DAA. The helicopter joined Route 1 near Cabin John, Maryland, and followed the Potomac River southbound at low altitude, passing the Key Bridge, Memorial Bridge, Tidal Basin, and Hains Point before continuing onto Route 4. At the same time, flight 5342 was approaching DCA on an instrument flight rules flight that had been uneventful during departure, cruise, and initial descent. The airplane was inbound from the south on a visual approach to runway 1 when the DCA tower controller asked the flight crew if they could accept runway 33 instead. After confirming landing performance, the crew accepted a circling approach to runway 33 and maneuvered the airplane to align with the runway 33 final approach path. While PAT25 was transitioning from Route 1 to Route 4 and flight 5342 was circling to land, the controller issued a traffic advisory to the helicopter crew about the airplane, which was south of the Woodrow Wilson Bridge. At this time, the airplane was about 6.5 nautical miles (about 7.5 statute miles) south of the helicopter’s position, and its exterior lights would have been visible in the dark among those of several other airplanes, which were on approach to runway 1 from the south. The instructor pilot onboard PAT25 stated that they had the traffic in sight and requested visual separation, which the controller approved. As the aircraft flightpaths converged near the runway 33 approach corridor about 1 1/2 minutes later (20 seconds before impact), the controller asked the helicopter crew whether they had the airplane in sight and instructed PAT25 to pass behind it; however, one of the helicopter pilots pressed the radio push-to-talk switch for 0.8 seconds while the controller was speaking, and this brief radio transmission blocked the helicopter crew from receiving the “pass behind” portion of the controller’s instruction. The instructor pilot onboard PAT25 again indicated that they had the airplane in sight and requested visual separation, which the controller approved. PAT25 continued southbound along Route 4 while flight 5342 descended on final approach for runway 33, and the aircraft collided over the Potomac River at an altitude about 278 ft above mean sea level (msl).
Probable cause:
We determined that the probable cause of this accident was the FAA’s placement of a helicopter route in close proximity to a runway approach path; their failure to regularly review and evaluate helicopter routes and available data, and their failure to act on recommendations to mitigate the risk of a midair collision near Ronald Reagan Washington National Airport; as well as the air traffic system’s overreliance on visual separation in order to promote efficient traffic flow without consideration for the limitations of the see-and-avoid concept. Also causal was the lack of effective pilot-applied visual separation by the helicopter crew, which resulted in a midair collision. Additional causal factors were the tower team’s loss of situation awareness and degraded performance due to the high workload of the combined helicopter and local control positions and the absence of a risk assessment process to identify and mitigate real-time operational risk factors, which resulted in misprioritization of duties, inadequate traffic advisories, and the lack of safety alerts to both flight crews. Also causal was the Army’s failure to ensure pilots were aware of the effects of error tolerances on barometric altimeters in their helicopters, which resulted in the crew flying above the maximum published helicopter route altitude. Contributing factors included:
• the limitations of the traffic awareness and collision alerting systems on both aircraft, which precluded effective alerting of the impending collision to the flight crews;
• an unsustainable airport arrival rate, increasing traffic volume with a changing fleet mix, and airline scheduling practices at DCA, which regularly strained the DCA ATCT workforce and degraded safety over time;
• the Army’s lack of a fully implemented safety management system, which should have identified and addressed hazards associated with altitude exceedances on the Washington, DC, helicopter routes;
• the FAA’s failure across multiple organizations to implement previous NTSB recommendations, including ADS-B In, and to follow and fully integrate its established safety management system, which should have led to several organizational and operational changes based on previously identified risks that were known to management; and
• the absence of effective data sharing and analysis among the FAA, aircraft operators, and other relevant organizations.
• the limitations of the traffic awareness and collision alerting systems on both aircraft, which precluded effective alerting of the impending collision to the flight crews;
• an unsustainable airport arrival rate, increasing traffic volume with a changing fleet mix, and airline scheduling practices at DCA, which regularly strained the DCA ATCT workforce and degraded safety over time;
• the Army’s lack of a fully implemented safety management system, which should have identified and addressed hazards associated with altitude exceedances on the Washington, DC, helicopter routes;
• the FAA’s failure across multiple organizations to implement previous NTSB recommendations, including ADS-B In, and to follow and fully integrate its established safety management system, which should have led to several organizational and operational changes based on previously identified risks that were known to management; and
• the absence of effective data sharing and analysis among the FAA, aircraft operators, and other relevant organizations.
Final Report: