Country
Crash of a Beechcraft B200 Super King Air in Gillam
Date & Time:
Apr 24, 2019 at 1823 LT
Operator:

Registration:
C-FRMV
Survivors:
Yes
Schedule:
Winnipeg – Churchill – Rankin Inlet
MSN:
BB-979
YOM:
1982
Flight number:
KEW202
Crew on board:
2
Crew fatalities:
Pax on board:
2
Pax fatalities:
Other fatalities:
Total fatalities:
0
Captain / Total hours on type:
1100.00
Copilot / Total hours on type:
1350
Circumstances:
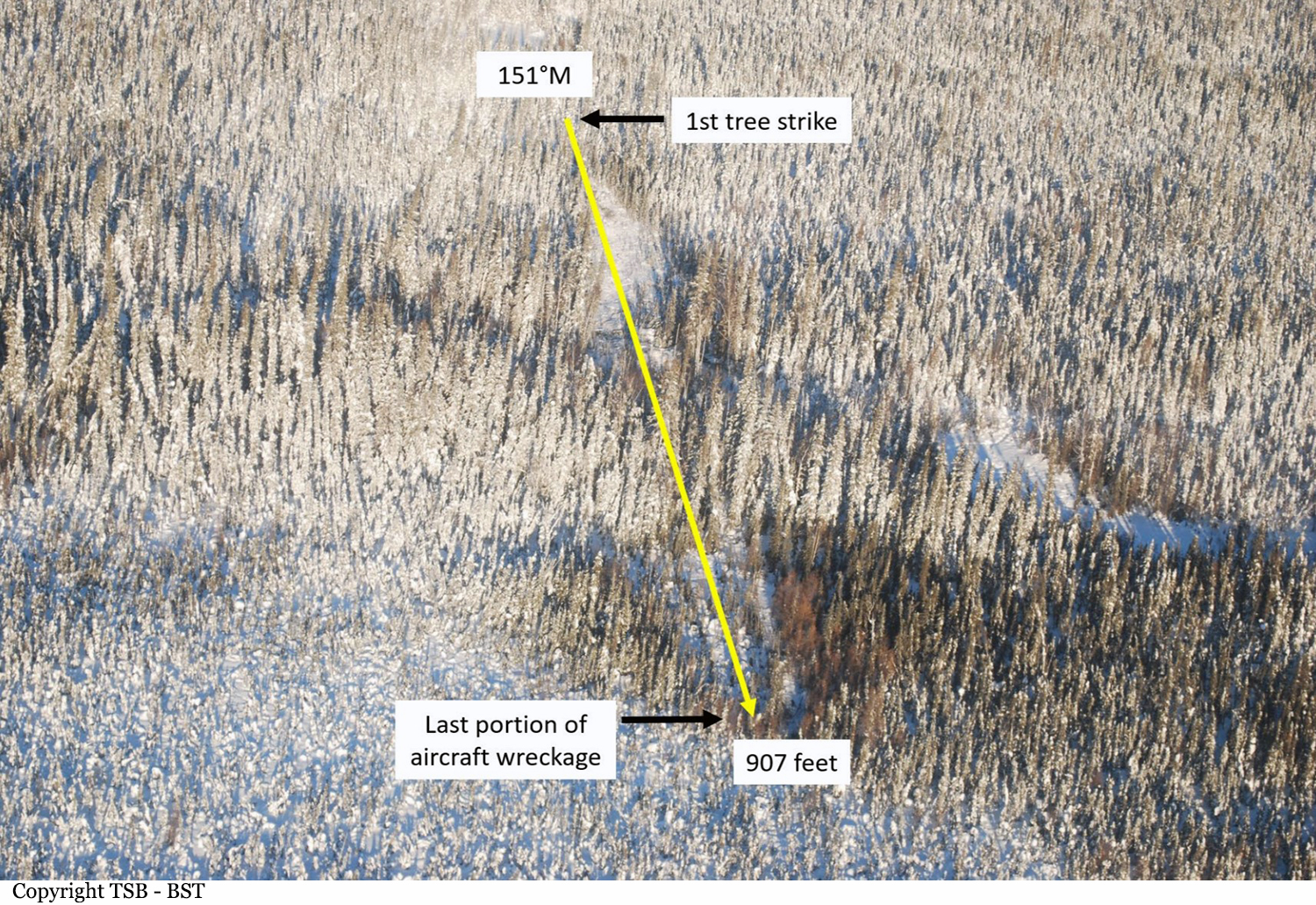
On 24 April 2019, the Keewatin Air LP Beechcraft B200 aircraft (registration C‑FRMV, serial number BB979), equipped to perform medical evacuation flights, was conducting an instrument flight rules positioning flight (flight KEW202), with 2 flight crew members and 2 flight nurses on board, from Winnipeg/James Armstrong Richardson International Airport, Manitoba, to Rankin Inlet Airport, Nunavut, with a stop at Churchill Airport, Manitoba. At 1814 Central Daylight Time, when the aircraft was cruising at flight level 250, the flight crew declared an emergency due to a fuel issue. The flight crew diverted to Gillam Airport, Manitoba, and initiated an emergency descent. During the descent, both engines flamed out. The flight crew attempted a forced landing on Runway 23, but the aircraft touched down on the frozen surface of Stephens Lake, 750 feet before the threshold of Runway 23. The landing gear was fully extended. The aircraft struck the rocky lake shore and travelled up the bank toward the runway area. It came to rest 190 feet before the threshold of Runway 23 at 1823:45 Central Daylight Time. None of the occupants was injured. The aircraft sustained substantial damage. The 406 MHz emergency locator transmitter activated. Emergency services responded. There was no fire.
Probable cause:
Findings as to causes and contributing factors:
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
1. When the captain asked if the aircraft was ready for the flight, the first officer replied that it was, not recalling that the aircraft required fuel.
2. While performing the FUEL QUANTITY item on the AFTER START checklist, the captain responded to the first officer’s prompt with the rote response that the fuel was sufficient, without looking at the fuel gauges.
3. The aircraft departed Winnipeg/James Armstrong Richardson International Airport with insufficient fuel on board to complete the planned flight.
4. The flight crew did not detect that there was insufficient fuel because the gauges had not been included in the periodic cockpit scans.
5. When the flight crew performed the progressive fuel calculation, they did not confirm the results against the fuel gauges, and therefore their attention was not drawn to the low-fuel state at a point that would have allowed for a safe landing.
6. Still feeling the effect of the startle response to the fuel emergency, the captain quickly became task saturated, which led to an uncoordinated response by the flight crew, delaying the turn toward Gillam Airport, and extending the approach.
7. The right engine lost power due to fuel exhaustion when the aircraft was 1 nautical mile from Runway 23. From that position, a successful forced landing on the intended runway was no longer possible and, as a result, the aircraft touched down on the ice surface of Stephens Lake, short of the runway.
Findings as to risk:
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
1. If procedures are not developed to instruct pilots on their roles and responsibilities during line indoctrination flights, there is a risk that flight crew members may not participate when expected, or may work independently towards different goals.
Other findings:
These items could enhance safety, resolve an issue of controversy, or provide a data point for future safety studies.
1. Because emergency medical services and the fire department were not notified immediately about the declared emergency, they were not on site before the aircraft arrived at Gillam Airport.
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
1. When the captain asked if the aircraft was ready for the flight, the first officer replied that it was, not recalling that the aircraft required fuel.
2. While performing the FUEL QUANTITY item on the AFTER START checklist, the captain responded to the first officer’s prompt with the rote response that the fuel was sufficient, without looking at the fuel gauges.
3. The aircraft departed Winnipeg/James Armstrong Richardson International Airport with insufficient fuel on board to complete the planned flight.
4. The flight crew did not detect that there was insufficient fuel because the gauges had not been included in the periodic cockpit scans.
5. When the flight crew performed the progressive fuel calculation, they did not confirm the results against the fuel gauges, and therefore their attention was not drawn to the low-fuel state at a point that would have allowed for a safe landing.
6. Still feeling the effect of the startle response to the fuel emergency, the captain quickly became task saturated, which led to an uncoordinated response by the flight crew, delaying the turn toward Gillam Airport, and extending the approach.
7. The right engine lost power due to fuel exhaustion when the aircraft was 1 nautical mile from Runway 23. From that position, a successful forced landing on the intended runway was no longer possible and, as a result, the aircraft touched down on the ice surface of Stephens Lake, short of the runway.
Findings as to risk:
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
1. If procedures are not developed to instruct pilots on their roles and responsibilities during line indoctrination flights, there is a risk that flight crew members may not participate when expected, or may work independently towards different goals.
Other findings:
These items could enhance safety, resolve an issue of controversy, or provide a data point for future safety studies.
1. Because emergency medical services and the fire department were not notified immediately about the declared emergency, they were not on site before the aircraft arrived at Gillam Airport.
Final Report:



Crash of a Beechcraft B200 Super King Air in Matsieng: 1 killed
Date & Time:
Mar 23, 2019 at 2020 LT
Operator:

Registration:
A2-MBM
Survivors:
No
Schedule:
Gaborone - Matsieng
MSN:
BB-1489
YOM:
1994
Crew on board:
1
Crew fatalities:
Pax on board:
0
Pax fatalities:
Other fatalities:
Total fatalities:
1
Circumstances:
Earlier in the afternoon the pilot was an uninvited guest at a private function that was held at the Matsieng Flying Club facility at Matsieng Aerodrome. In a statement, the Matsieng Flying Club reported that it was rumored that the pilot was involved in a domestic dispute earlier in the afternoon. At 2015LT the aircraft approached Matsieng Aerodrome from the direction of Sir Seretse Khama Airport and made a number of low level fly passes from different directions past the Club facilities next to the Air Traffic Control tower. An immediate evacuation of the club premises was ordered. The final extreme low level run by the aircraft along runway 36 resulted in an impact with the Matsieng Flying Club facility at ground level. The Club facility and Matsieng ATC tower was destroyed on impact. The post impact fire destroyed 13 parked vehicles. The emergency services of the Kgatleng District Council were on the scene within minutes to attend to the post-impact fire and distress. These response actions are to be commended. It is believed that the pilot had no permission to fly the aircraft involved. Sole on board, he was killed.
Probable cause:
Pilot suicide suspected.


Crash of a Beechcraft B200 Super King in Whatì: 2 killed
Date & Time:
Jan 30, 2019 at 0915 LT
Operator:

Registration:
C-GTUC
Survivors:
No
Schedule:
Yellowknife – Whatì – Wekweèti – Ekati
MSN:
BB-268
YOM:
1977
Flight number:
8T503
Crew on board:
2
Crew fatalities:
Pax on board:
0
Pax fatalities:
Other fatalities:
Total fatalities:
2
Captain / Total hours on type:
1712.00
Copilot / Total hours on type:
330
Aircraft flight hours:
20890
Aircraft flight cycles:
18863
Circumstances:
At 0851 Mountain Standard Time on 30 January 2019, the Air Tindi Ltd. Beechcraft King Air 200 aircraft (registration C-GTUC, serial number BB-268) departed Yellowknife Airport (CYZF), Northwest Territories, as flight TIN503, on an instrument flight rules flight itinerary to Whatì Airport (CEM3), Northwest Territories, with 2 crew members on board. At 0912, as the aircraft began the approach to CEM3, it departed controlled flight during its initial descent from 12 000 feet above sea level, and impacted terrain approximately 21 nautical miles east-southeast of CEM3, at an elevation of 544 feet above sea level. The Canadian Mission Control Centre received a signal from the aircraft’s 406 MHz emergency locator transmitter and notified the Joint Rescue Coordination Centre in Trenton, Ontario. Search and rescue technicians arrived on site approximately 6 hours after the accident. The 2 flight crew members received fatal injuries on impact. The aircraft was destroyed.
Probable cause:
Findings as to causes and contributing factors:
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
- For undetermined reasons, the left-side attitude indicator failed in flight.
- Although just before take off the crew acknowledged that the right-side attitude indicator was not operative, they expected it to become operative at some point in the flight. As a result, they did not refer to the minimum equipment list, and departed into instrument meteorological conditions with an inoperative attitude indicator.
- The crew’s threat and error management was not effective in mitigating the risk associated with the unserviceable right-side attitude indicator.
- The crew’s crew resource management was not effective, resulting in a breakdown in verbal communication, a loss of situation awareness, and the aircraft entering an unsafe condition.
- The captain did not have recent experience in flying partial panel. As a result, the remaining instruments were not used effectively and the aircraft departed controlled flight and entered a spiral dive.
- The captain and first officer likely experienced spatial disorientation.
- Once the aircraft emerged below the cloud layer at approximately 2000 feet above ground, the crew were unable to recover control of the aircraft in enough time and with enough altitude to avoid an impact with terrain.
Findings as to risk:
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
- If flight crews do not use the guidance material provided in the minimum equipment list when aircraft systems are unserviceable, there is a risk that the aircraft will be operated without systems that are critical to safe aircraft operation.
- If flight crews do not use all available resources at their disposal, a loss in situation awareness can occur, which can increase the risk of an accident.
Other findings:
These items could enhance safety, resolve an issue of controversy, or provide a data point for future safety studies.
- A review of Air Tindi Ltd.'s pilot training program revealed that all regulatory requirements were being met or exceeded.
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
- For undetermined reasons, the left-side attitude indicator failed in flight.
- Although just before take off the crew acknowledged that the right-side attitude indicator was not operative, they expected it to become operative at some point in the flight. As a result, they did not refer to the minimum equipment list, and departed into instrument meteorological conditions with an inoperative attitude indicator.
- The crew’s threat and error management was not effective in mitigating the risk associated with the unserviceable right-side attitude indicator.
- The crew’s crew resource management was not effective, resulting in a breakdown in verbal communication, a loss of situation awareness, and the aircraft entering an unsafe condition.
- The captain did not have recent experience in flying partial panel. As a result, the remaining instruments were not used effectively and the aircraft departed controlled flight and entered a spiral dive.
- The captain and first officer likely experienced spatial disorientation.
- Once the aircraft emerged below the cloud layer at approximately 2000 feet above ground, the crew were unable to recover control of the aircraft in enough time and with enough altitude to avoid an impact with terrain.
Findings as to risk:
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
- If flight crews do not use the guidance material provided in the minimum equipment list when aircraft systems are unserviceable, there is a risk that the aircraft will be operated without systems that are critical to safe aircraft operation.
- If flight crews do not use all available resources at their disposal, a loss in situation awareness can occur, which can increase the risk of an accident.
Other findings:
These items could enhance safety, resolve an issue of controversy, or provide a data point for future safety studies.
- A review of Air Tindi Ltd.'s pilot training program revealed that all regulatory requirements were being met or exceeded.
Final Report:

Crash of a Beechcraft B200 Super King Air off Kake: 3 killed
Date & Time:
Jan 29, 2019 at 1811 LT
Operator:

Registration:
N13LY
Survivors:
No
Schedule:
Anchorage - Kake
MSN:
BB-1718
YOM:
2000
Crew on board:
1
Crew fatalities:
Pax on board:
2
Pax fatalities:
Other fatalities:
Total fatalities:
3
Captain / Total hours on type:
1644.00
Aircraft flight hours:
5226
Circumstances:
The pilot of the medical transport flight had been cleared by the air traffic controller for the instrument approach and told by ATC to change to the advisory frequency, which the pilot acknowledged. After crossing the initial approach fix on the RNAV approach, the airplane began a gradual descent and continued northeast towards the intermediate fix. Before reaching the intermediate fix, the airplane entered a right turn and began a rapid descent, losing about 2,575 ft of altitude in 14 seconds; radar returns were then lost. A witness at the destination airport, who was scheduled to meet the accident airplane, observed the pilot-controlled runway lights illuminate. When the airplane failed to arrive, she contacted the company to inquire about the overdue airplane. The following day, debris was found floating on the surface of the ocean. About 48 days later, after an extensive underwater search, the heavily fragmented wreckage was located on the ocean floor at a depth of about 500 ft. A postaccident examination of the engines revealed contact signatures consistent with the engines developing power at the time of impact and no evidence of mechanical malfunctions or failures that would have precluded normal operation. A postaccident examination of the airframe revealed about a 10° asymmetric flap condition; however, significant impact damage was present to the flap actuator flex drive cables and flap actuators, indicating the flap actuator measurements were likely not a reliable source of preimpact flap settings. In addition, it is unlikely that a 10° asymmetric flap condition would result in a loss of control. The airplane was equipped with a total of 5 seats and 5 restraints. Of the three restraints recovered, none were buckled. The unbuckled restraints could suggest an emergency that required crewmembers to be up and moving about the cabin; however, the reason for the unbuckled restraints could not be confirmed. While the known circumstances of the accident are consistent with a loss of control event, the factual information available was limited because the wreckage in its entirety was not recovered, the CVR recording did not contain the accident flight, no non-volatile memory was recovered from the accident airplane, and no autopsy or toxicology of the pilot could be performed; therefore, the reason for the loss of control could not be determined. Due to the limited factual information that was available, without a working CVR there is little we know about this accident.
Probable cause:
A loss of control for reasons that could not be determined based on the available information.
Final Report:




